

Resolution of Chronic Migraine Headaches and Improvement in Cervical Spine Kyphosis Following Chiropractic BioPhysics® (CBP®) Treatment: A Case Report With a Seven-Month Follow-Up
- PMID: 39329038
- PMCID: PMC11427026
- DOI: 10.7759/cureus.69935
Resolution of Chronic Migraine Headaches and Improvement in Cervical Spine Kyphosis Following Chiropractic BioPhysics® (CBP®) Treatment: A Case Report With a Seven-Month Follow-Up
Abstract
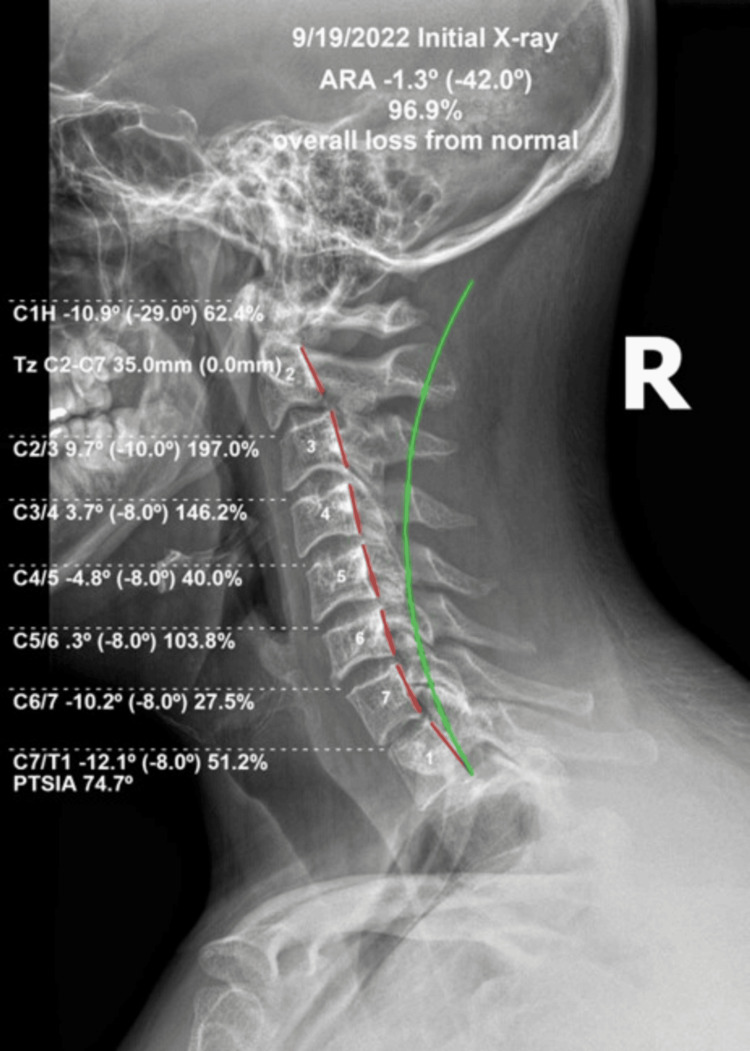
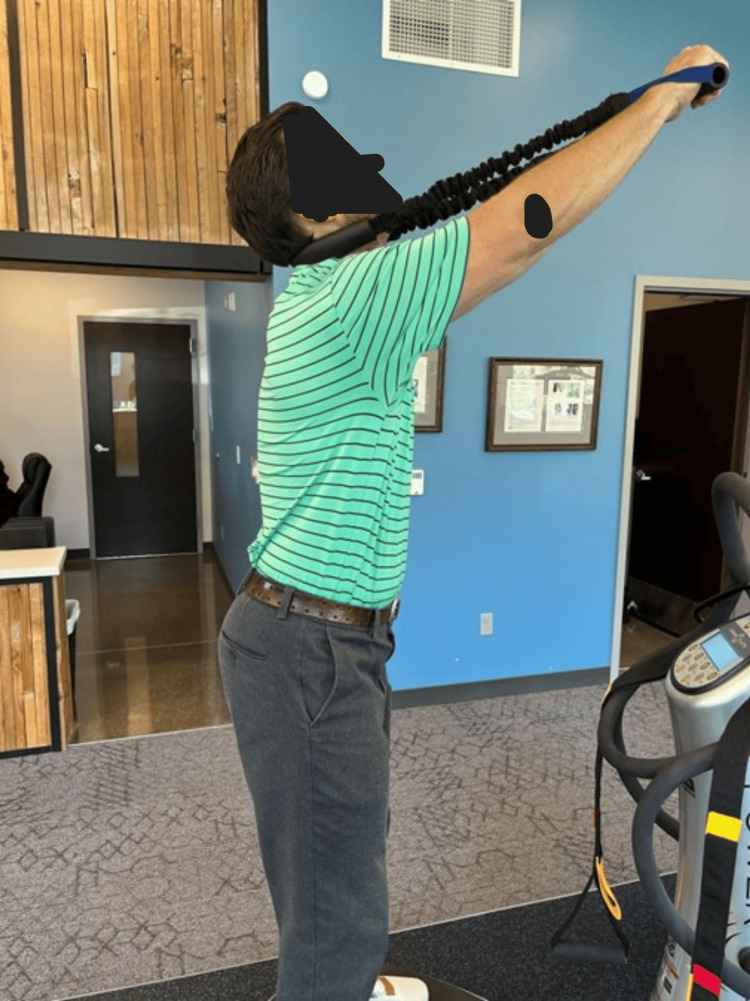
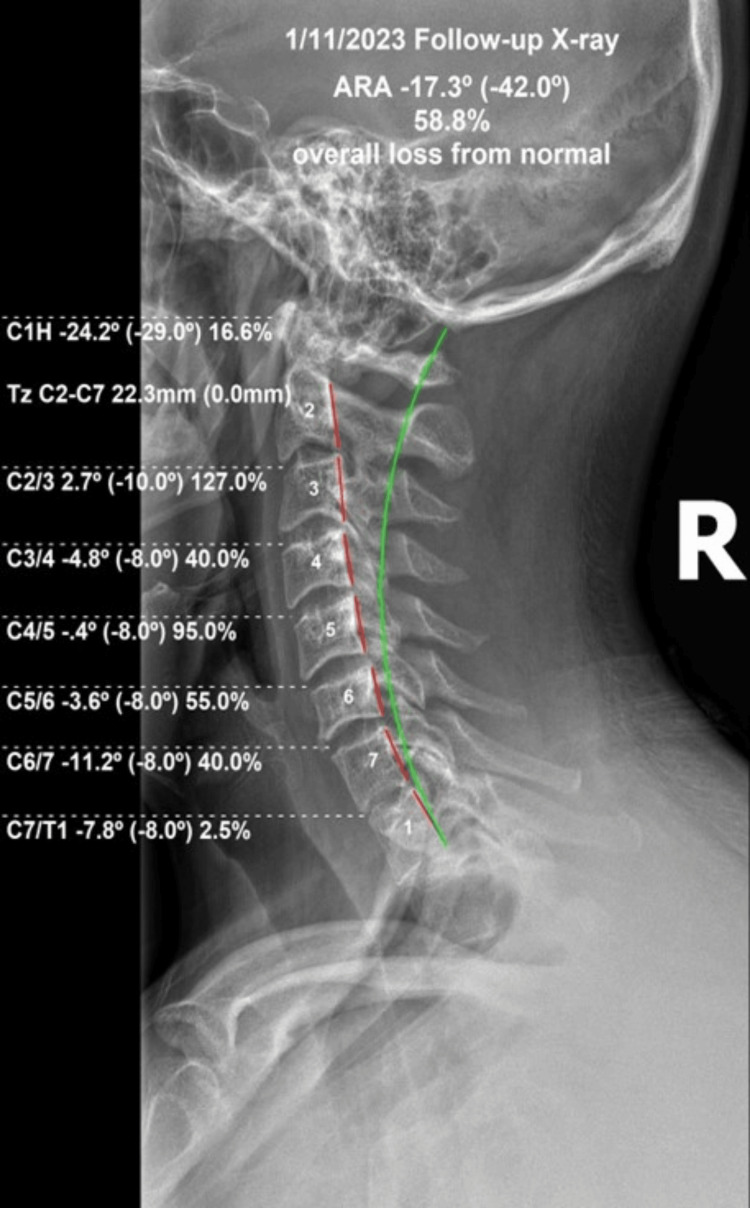
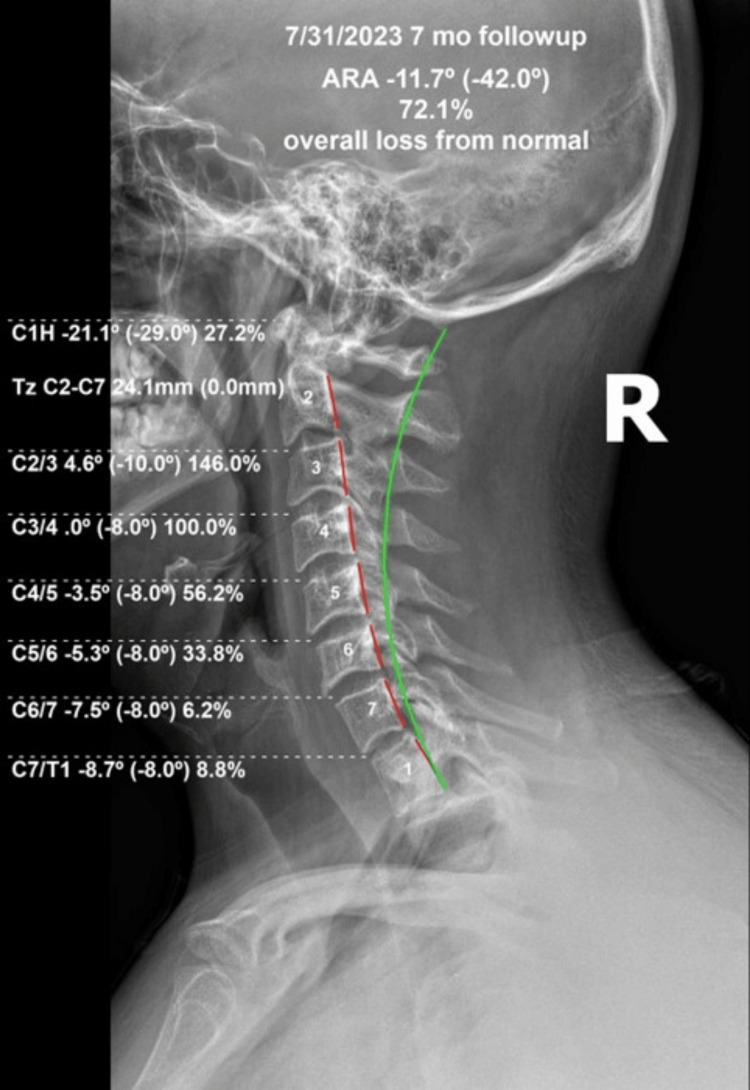
We present a chronic migraine (CM) patient demonstrating significant improvement in subjective and objective reported outcome measures with deeper cervical lordosis parameters and reduced forward head posture on radiographs. A 29-year-old male suffered from CM reporting significant pain and disability with aural, sensory, and motor disturbances during the migraine headaches. Aura with visual disturbances, abnormal facial and extremity sensation, sporadic motor weakness, and other signs of CM were found in the patient's history since age 10. The patient reported previous physical therapy, manual chiropractic, and over-the-counter medications. Migraine-specific prescriptions without long-term reduction in pain and disability were reported. The pain and suffering had been reported to be worsening, and he sought Chiropractic BioPhysics® (CBP®) spine and postural rehabilitation protocols. These protocols were used to increase cervical lordosis, reduce coronal imbalances, increase mobility, and create better posture. These protocols include specific prescriptions based on radiography for postural exercises, postural mirror image® (MI®)traction, and specific spinal manipulative therapy (SMT) focused on posture. All outcome measures improved with the resolution of all initial symptoms of CM. There was a 16° improvement in cervical lordosis, a 30% decrease in headache disability, and additional improvements. These improvements were maintained at a seven-month follow-up during which the patient received infrequent maintenance treatments. This successful treatment of a patient with CM with long-term follow-up adds to evidence that CBP® spinal structural rehabilitation may prove effective and serve as a possible tool for clinicians, physicians, and therapists to treat CM.
Keywords: cervical lateral radiograph; cervical lordosis; chiropractic biophysics; headache; migraine; sagittal balance; spine alignment.
Copyright © 2024, Oakley et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: MOF and TJW have no conflicts of interest. PAO is a compensated consultant for CBP NonProfit, Inc.; JWH is a compensated instructor and researcher for CBP® Seminars; DEH is the CEO of Chiropractic BioPhysics® (CBP®) and provides post-graduate education and rehabilitation devices to health care providers/physicians. DEH is the president of CBP® NonProfit, Inc., a not-for-profit spine research foundation. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

Similar articles
-
Resolution of Sporadic Hemiplegic Migraine by Correcting a Cervical Spine Kyphosis Utilizing the Chiropractic BioPhysics® (CBP®) Technique: A Case Report With Long-Term Follow-Up.Cureus. 2024 Jul 3;16(7):e63774. doi: 10.7759/cureus.63774. eCollection 2024 Jul. Cureus. 2024. PMID: 38974394 Free PMC article.
-
Reducing Chronic Spine Pain in an Adult Male by Decreasing Lumbar Scoliosis and Increasing Cervical Lordosis Using Chiropractic BioPhysics® Protocols: A 26-Month Follow-Up Case Report.Cureus. 2024 Sep 1;16(9):e68393. doi: 10.7759/cureus.68393. eCollection 2024 Sep. Cureus. 2024. PMID: 39224496 Free PMC article.
-
Improvement in Chronic Low Back and Intermittent Chronic Neck Pain, Disability, and Improved Spine Parameters Using Chiropractic BioPhysics® Rehabilitation After 5 Years of Failed Chiropractic Manipulation: A Case Report and 1-Year Follow-Up.Healthcare (Basel). 2025 Apr 3;13(7):814. doi: 10.3390/healthcare13070814. Healthcare (Basel). 2025. PMID: 40218115 Free PMC article.
-
Structural rehabilitation of the cervical lordosis and forward head posture: a selective review of Chiropractic BioPhysics® case reports.J Phys Ther Sci. 2022 Nov;34(11):759-771. doi: 10.1589/jpts.34.759. Epub 2022 Nov 1. J Phys Ther Sci. 2022. PMID: 36337218 Free PMC article. Review.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
References
-
- Migraine: epidemiology, burden, and comorbidity. Burch RC, Buse DC, Lipton RB. Neurol Clin. 2019;37:631–649. - PubMed
-
- Influences of genetic and environmental factors on chronic migraine: a narrative review. Yeh PK, An YC, Hung KS, Yang FC. Curr Pain Headache Rep. 2024;28:169–180. - PubMed
-
- Prevalence and burden of migraine in the United States: a systematic review. Cohen F, Brooks CV, Sun D, Buse DC, Reed ML, Fanning KM, Lipton RB. Headache. 2024;64:516–532. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous