

Neoadjuvant therapy versus upfront surgery in resectable pancreatic cancer: reconstructed patient-level meta-analysis of randomized clinical trials
- PMID: 39329454
- PMCID: PMC11428068
- DOI: 10.1093/bjsopen/zrae087
Neoadjuvant therapy versus upfront surgery in resectable pancreatic cancer: reconstructed patient-level meta-analysis of randomized clinical trials
Abstract
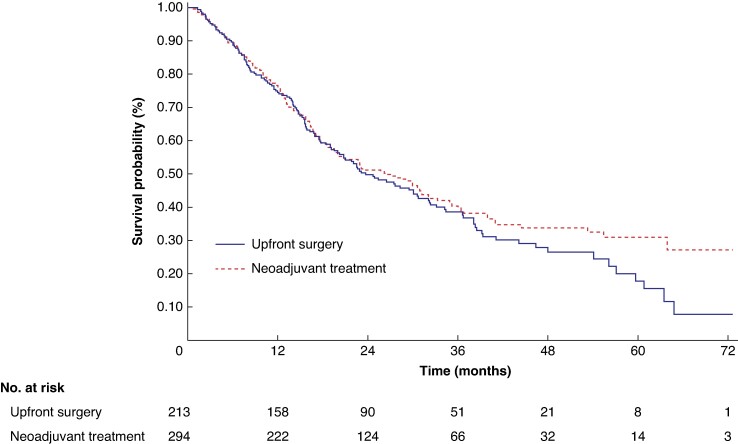
Background: Neoadjuvant treatment has shown promising results in patients with borderline resectable pancreatic ductal adenocarcinoma. The potential benefits of neoadjuvant treatment on long-term overall survival in patients with resectable pancreatic ductal adenocarcinoma have not yet been established. The aim of this study was to compare long-term overall survival of patients with resectable pancreatic ductal adenocarcinoma based on whether they received neoadjuvant treatment or underwent upfront surgery.
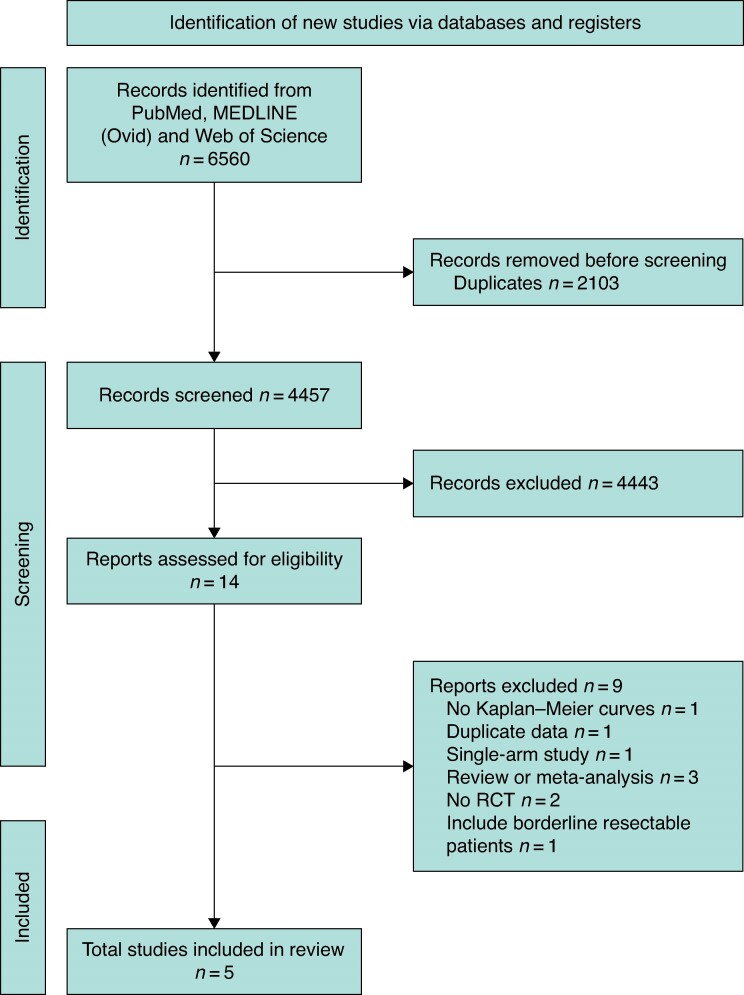
Methods: A systematic review including randomized clinical trials on the overall survival outcomes between neoadjuvant treatment and upfront surgery in patients with resectable pancreatic ductal adenocarcinoma was conducted up to 1 August 2023 from PubMed, MEDLINE and Web of Science databases. Patient-level survival data was extracted and reconstructed from available Kaplan-Meier curves. A frequentist one-stage meta-analysis was employed, using Cox-based models and a non-parametric method (restricted mean survival time), to assess the difference in overall survival between groups. A Bayesian meta-analysis was also conducted.
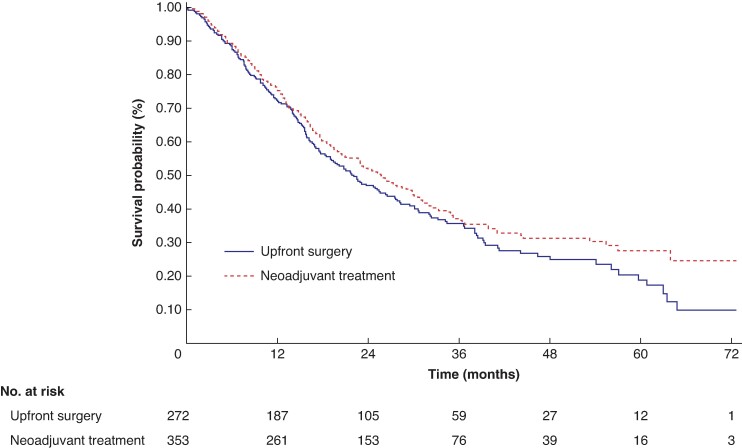
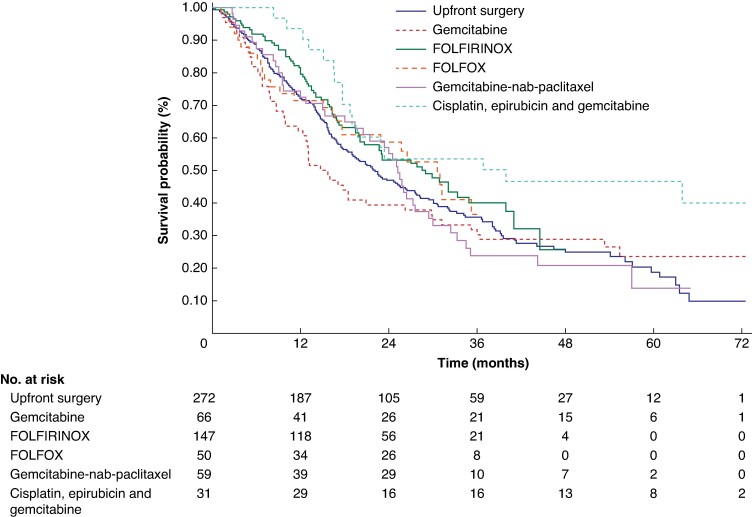
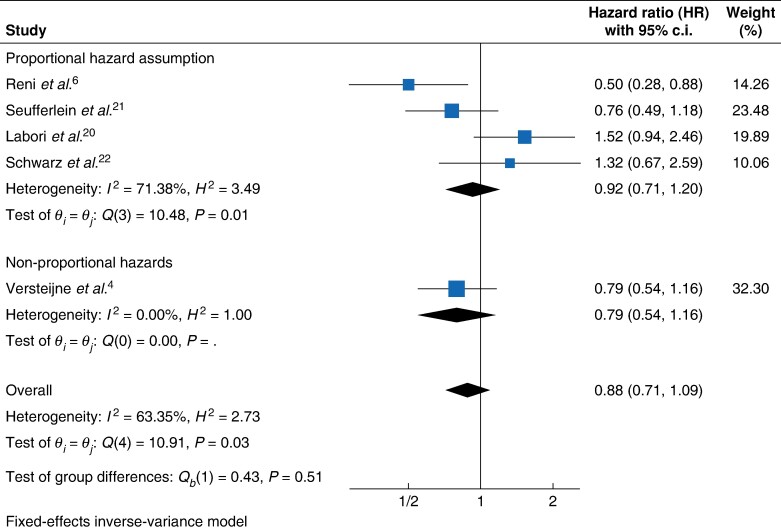
Results: Five randomized clinical trials comprising 625 patients were included. Among patients with resectable pancreatic ductal adenocarcinoma, neoadjuvant treatment was not significantly associated with a reduction in the hazard of death compared with upfront surgery (shared frailty HR 0.88, 95% c.i. 0.72 to 1.08, P = 0.223); this result was consistent in the non-parametric restricted mean survival time model (+2.41 months, 95% c.i. -1.22 to 6.04, P < 0.194), in the sensitivity analysis that excluded randomized clinical trials with a high risk of bias (shared frailty HR 0.91 (95% c.i. 0.72 to 1.15; P = 0.424)) and in the Bayesian analysis with a posterior shared frailty HR of 0.86 (95% c.i. 0.70 to 1.05).
Conclusion: Neoadjuvant treatment does not demonstrate a survival advantage over upfront surgery for patients with resectable pancreatic ductal adenocarcinoma.
© The Author(s) 2024. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Figures
References
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014;74:2913–2921 - PubMed
-
- National Comprehensive Cancer Network . Pancreatic Cancer (Version 1. 2022). https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf (accessed January 2024)
-
- Versteijne E, van Dam JL, Suker M, Janssen QP, Groothuis K, Akkermans-Vogelaar JM et al. Neoadjuvant chemoradiotherapy versus upfront surgery for resectable and borderline resectable pancreatic cancer: long-term results of the Dutch Randomized PREOPANC trial. J Clin Oncol 2022;40:1220–1230 - PubMed
-
- Mokdad AA, Minter RM, Zhu H, Augustine MM, Porembka MR, Wang SC et al. Neoadjuvant therapy followed by resection versus upfront resection for resectable pancreatic cancer: a propensity score matched analysis. J Clin Oncol 2016;35:515–522 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
