

An Insert Goniometer Can Help Select the Optimal Insert Thickness When Performing Kinematically Aligned Total Knee Arthroplasty with a Medial 1:1 Ball-in-Socket and Lateral Flat Surface Insert and Posterior Cruciate Ligament Retention
- PMID: 39329652
- PMCID: PMC11444139
- DOI: 10.3390/bioengineering11090910
An Insert Goniometer Can Help Select the Optimal Insert Thickness When Performing Kinematically Aligned Total Knee Arthroplasty with a Medial 1:1 Ball-in-Socket and Lateral Flat Surface Insert and Posterior Cruciate Ligament Retention
Abstract
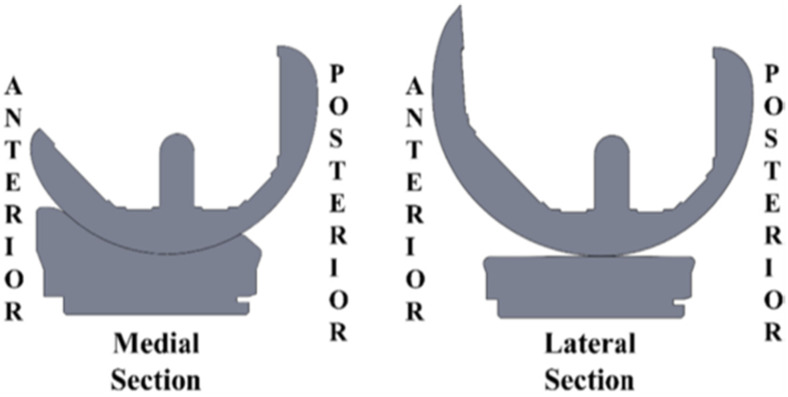
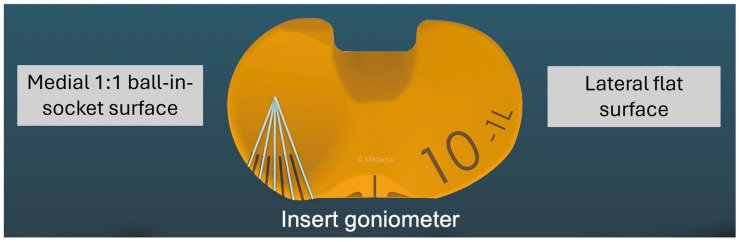
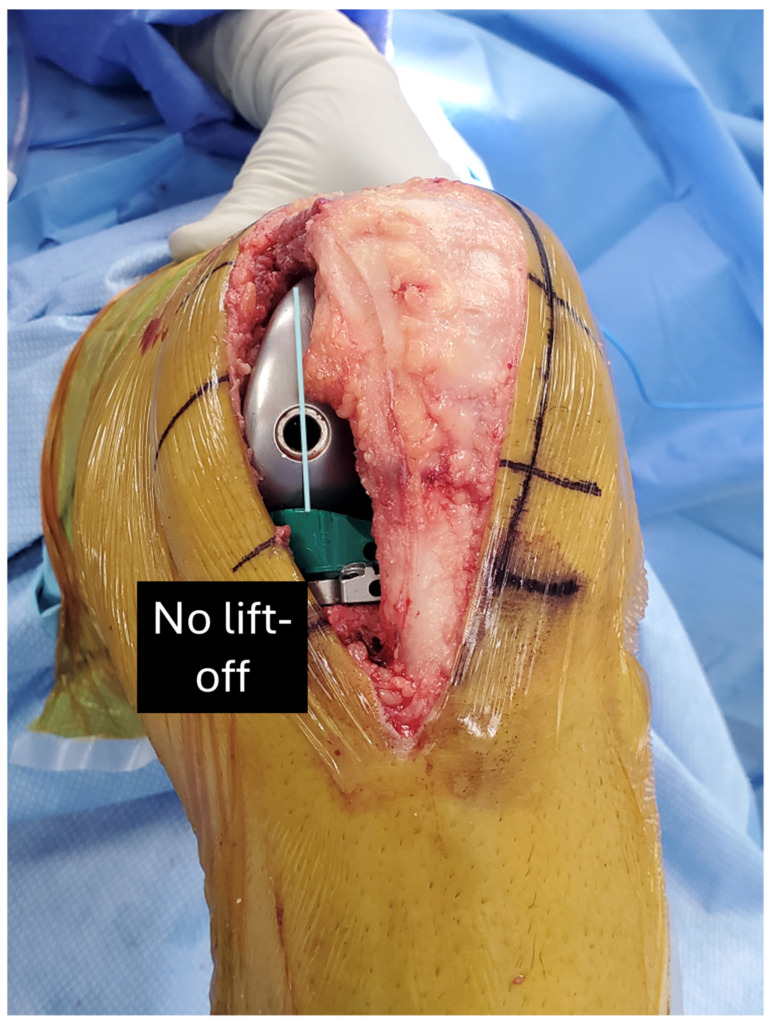
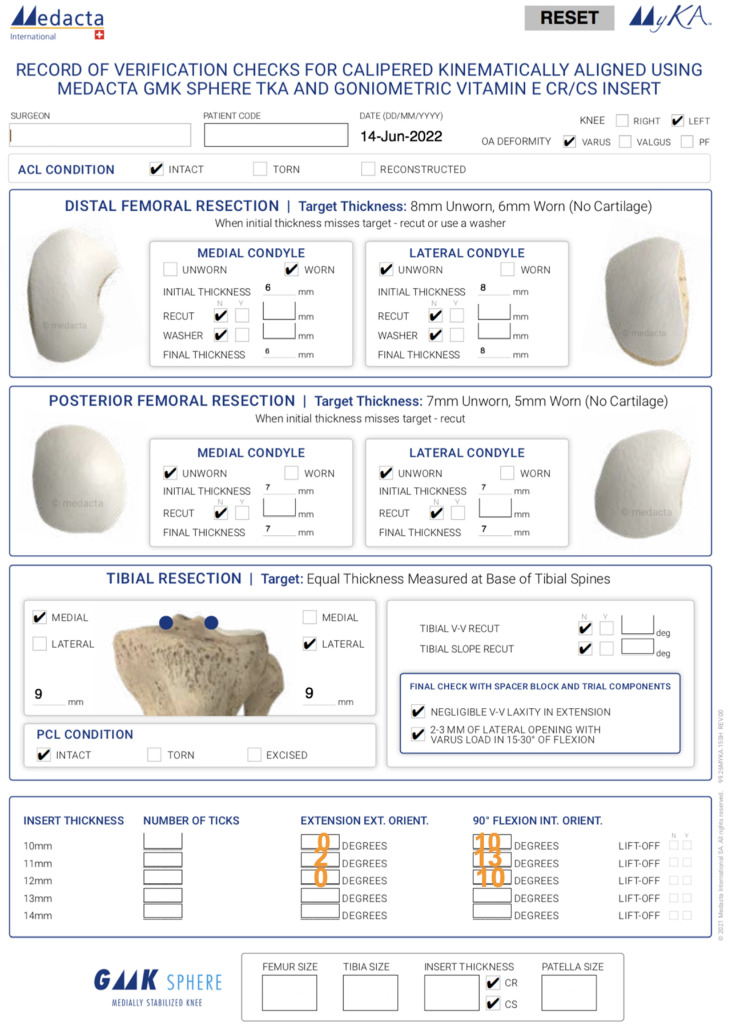
Current surgical practices in total knee arthroplasty (TKA) have advanced and include significant changes and improvements in alignment philosophies, femorotibial implant conformities, and ligament management to replicate in vivo knee kinematics. While corrective measures have emphasized sagittal plane alignment to restore normal flexion-extension (F-E) motion and coronal plane ligament balance, internal-external (I-E) rotation kinematics in the axial plane have been largely neglected. Recent in vivo evidence indicates that the combination of factors necessary to closely restore native tibial rotation as the knee flexes and extends is kinematic alignment (KA), which resurfaces the patient's pre-arthritic knee without releasing ligaments, an insert with medial 1:1 ball-in-socket conformity and a lateral flat surface, and posterior cruciate ligament (PCL) retention. However, the inherent anterior-posterior (A-P) stability provided by the medial 1:1 ball-in-socket limits the surgeon's ability to select the correct insert thickness using manual laxity testing. Accordingly, this review presents the design and validation of an instrument called an insert goniometer that measures I-E tibial rotation for inserts that differ in thickness by 1 mm and uses rotation limits at extension and 90° flexion to select the optimal insert thickness. The optimal thickness is the one that provides the greatest external tibial orientation in extension and internal tibial orientation at 90° flexion without lift-off of the insert.
Keywords: external tibial rotation; internal tibial rotation; quadriceps line of force; screw home mechanism; tibiofemoral kinematics; total knee replacement.
Conflict of interest statement
S.M.H. is a paid consultant, a paid speaker, and receives royalties from Medacta International. A.J.N. is a paid consultant and receives royalties from Medacta International. M.L.H. receives research support from Medacta USA, Inc. and is on the editorial board of the Journal of Biomechanics.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
