

Current Approaches for the Prevention and Treatment of Acute and Chronic GVHD
- PMID: 39329708
- PMCID: PMC11431085
- DOI: 10.3390/cells13181524
Current Approaches for the Prevention and Treatment of Acute and Chronic GVHD
Abstract
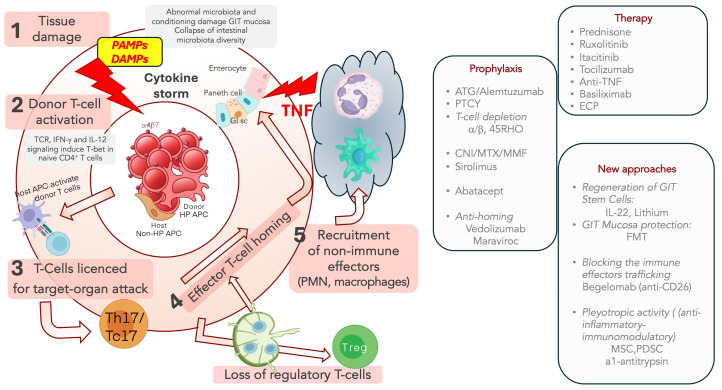
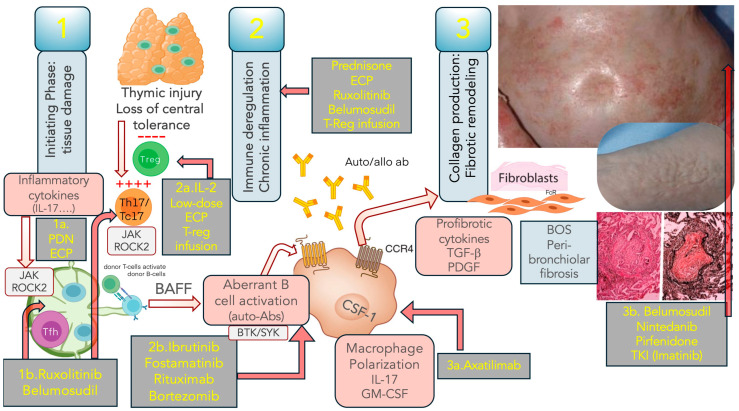
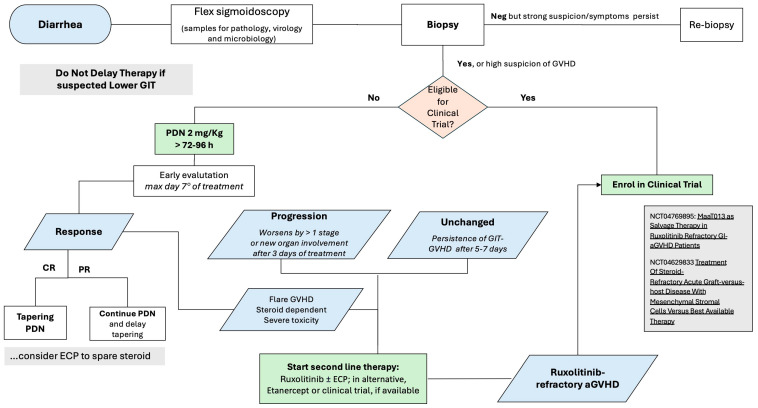
Whereas aGVHD has strong inflammatory components, cGVHD displays autoimmune and fibrotic features; incidence and risk factors are similar but not identical; indeed, the aGVHD is the main risk factor for cGVHD. Calcineurin Inhibitors (CNI) with either Methotrexate (MTX) or Mycophenolate (MMF) still represent the standard prophylaxis in HLA-matched allogeneic stem cell transplantation (HSCT); other strategies focused on ATG, Post-Transplant Cyclophosphamide (PTCy), Abatacept and graft manipulation. Despite the high rate, first-line treatment for aGVHD is represented by corticosteroids, and Ruxolitinib is the standard second-line therapy; investigational approaches include Microbiota transplant and the infusion of Mesenchymal stem cells. GVHD is a pleiotropic disease involving any anatomical district; also, Ruxolitinib represents the standard for steroid-refractory cGVHD in this setting. It is a pleiotropic disease involving any anatomical district; also, Ruxolitinib represents the standard for steroid-refractory cGVHD in this setting. Extracorporeal Photopheresis (ECP) is still an option used for steroid refractoriness or to achieve a steroid-sparing. For Ruxolitinib-refractory cGVHD, Belumosudil and Axatilimab represent the most promising agents. Bronchiolitis obliterans syndrome (BOS) still represents a challenge; among the compounds targeting non-immune effectors, Alvelestat, a Neutrophil elastase inhibitor, seems promising in BOS. Finally, in both aGVHD and cGVHD, the association of biological markers with specific disease manifestations could help refine risk stratification and the availability of reliable biomarkers for specific treatments.
Keywords: graft versus host prophylaxis; graft versus host treatment; transplantation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Treatment of steroid-refractory acute/chronic graft versus host disease: A single-center real-world experience of ruxolitinib in combination with extracorporeal photopheresis in a high-risk population.Leuk Res. 2024 Dec;147:107611. doi: 10.1016/j.leukres.2024.107611. Epub 2024 Oct 29. Leuk Res. 2024. PMID: 39500129
-
Ruxolitinib for pediatric acute and chronic graft-versus-host disease: a single-center retrospective study of efficacy and safety.Ann Hematol. 2025 Jan;104(1):753-760. doi: 10.1007/s00277-025-06225-0. Epub 2025 Feb 4. Ann Hematol. 2025. PMID: 39903278 Free PMC article.
-
Calcineurin Inhibitors Replacement by Ruxolitinib as Graft-versus-Host Disease Prophylaxis for Patients after Allogeneic Stem Cell Transplantation.Biol Blood Marrow Transplant. 2020 May;26(5):e128-e133. doi: 10.1016/j.bbmt.2020.01.012. Epub 2020 Jan 23. Biol Blood Marrow Transplant. 2020. PMID: 31982545
-
[Recent advances in prevention and treatment of chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation].Rinsho Ketsueki. 2024;65(5):401-411. doi: 10.11406/rinketsu.65.401. Rinsho Ketsueki. 2024. PMID: 38825520 Review. Japanese.
-
Efficacy and safety of ruxolitinib for steroid-refractory graft-versus-host disease: Systematic review and meta-analysis of randomised and non-randomised studies.PLoS One. 2022 Jul 29;17(7):e0271979. doi: 10.1371/journal.pone.0271979. eCollection 2022. PLoS One. 2022. PMID: 35905125 Free PMC article.
Cited by
-
Advancing therapeutic strategies for graft-versus-host disease by targeting gut microbiome dynamics in allogeneic hematopoietic stem cell transplantation: current evidence and future directions.Mol Med. 2025 Jan 3;31(1):2. doi: 10.1186/s10020-024-01060-x. Mol Med. 2025. PMID: 39754054 Free PMC article. Review.
-
Comprehensive Review of Early and Late Toxicities in CAR T-Cell Therapy and Bispecific Antibody Treatments for Hematologic Malignancies.Cancers (Basel). 2025 Jan 17;17(2):282. doi: 10.3390/cancers17020282. Cancers (Basel). 2025. PMID: 39858064 Free PMC article. Review.
-
JAK2 Inhibitors and Emerging Therapies in Graft-Versus-Host Disease: Current Perspectives and Future Directions.Biomedicines. 2025 Jun 23;13(7):1527. doi: 10.3390/biomedicines13071527. Biomedicines. 2025. PMID: 40722603 Free PMC article. Review.
-
Donor macrophage pyroptosis contributes to the development of aGVHD.Sci China Life Sci. 2025 Jun 16. doi: 10.1007/s11427-024-2908-8. Online ahead of print. Sci China Life Sci. 2025. PMID: 40528147
-
Decoy cells detected in the urine of a patient with complex karyotype Myelodysplastic neoplasms who underwent umbilical cord blood transplantation: a case report.BMC Nephrol. 2024 Nov 5;25(1):397. doi: 10.1186/s12882-024-03838-x. BMC Nephrol. 2024. PMID: 39501185 Free PMC article.
References
-
- Arai S., Arora M., Wang T., Spellman S.R., He W., Couriel D.R., Urbano-Ispizua A., Cutler C.S., Bacigalupo A.A., Battiwalla M., et al. Increasing incidence of chronic graft-versus-host disease in allogeneic transplantation: A report from the Center for International Blood and Marrow Transplant Research. Biol. Blood Marrow Transplant. 2015;21:266–274. doi: 10.1016/j.bbmt.2014.10.021. - DOI - PMC - PubMed
-
- Harris A.C., Young R., Devine S., Hogan W.J., Ayuk F., Bunworasate U., Chanswangphuwana C., Efebera Y.A., Holler E., Litzow M., et al. International, Multicenter Standardization of Acute Graft-versus-Host Disease Clinical Data Collection: A Report from the Mount Sinai Acute GVHD International Consortium. Biol. Blood Marrow Transplant. 2016;22:4–10. doi: 10.1016/j.bbmt.2015.09.001. - DOI - PMC - PubMed
-
- Filipovich A.H., Weisdorf D., Pavletic S., Socie G., Wingard J.R., Lee S.J., Martin P., Chien J., Przepiorka D., Couriel D., et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2005;11:945–956. doi: 10.1016/j.bbmt.2005.09.004. - DOI - PubMed
-
- Jagasia M.H., Greinix H.T., Arora M., Williams K.M., Wolff D., Cowen E.W., Palmer J., Weisdorf D., Treister N.S., Cheng G.-S., et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2015;21:389–401.e1. doi: 10.1016/j.bbmt.2014.12.001. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
