

Current Approaches for the Prevention and Treatment of Acute and Chronic GVHD
- PMID: 39329708
- PMCID: PMC11431085
- DOI: 10.3390/cells13181524
Current Approaches for the Prevention and Treatment of Acute and Chronic GVHD
Abstract
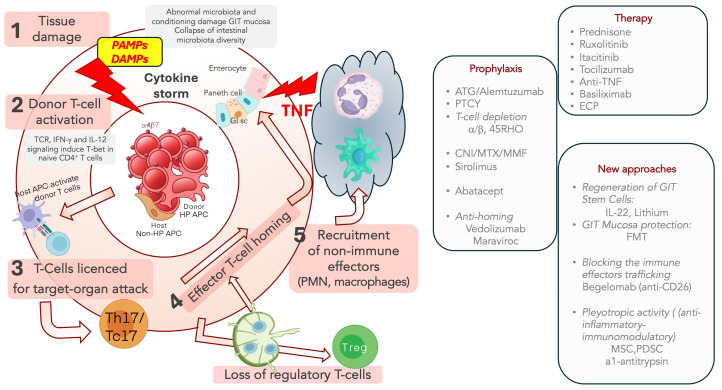
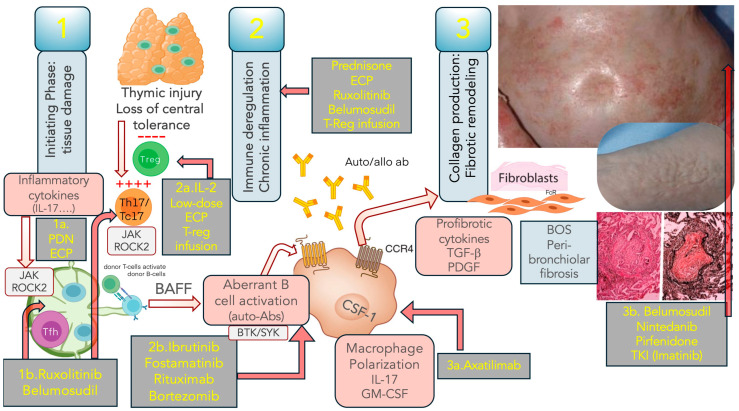
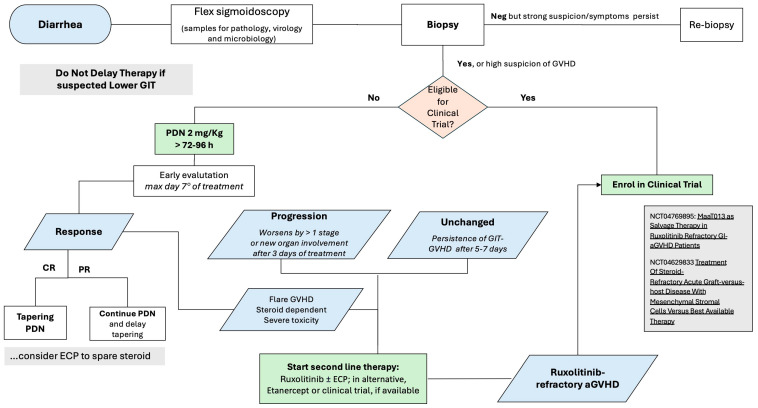
Whereas aGVHD has strong inflammatory components, cGVHD displays autoimmune and fibrotic features; incidence and risk factors are similar but not identical; indeed, the aGVHD is the main risk factor for cGVHD. Calcineurin Inhibitors (CNI) with either Methotrexate (MTX) or Mycophenolate (MMF) still represent the standard prophylaxis in HLA-matched allogeneic stem cell transplantation (HSCT); other strategies focused on ATG, Post-Transplant Cyclophosphamide (PTCy), Abatacept and graft manipulation. Despite the high rate, first-line treatment for aGVHD is represented by corticosteroids, and Ruxolitinib is the standard second-line therapy; investigational approaches include Microbiota transplant and the infusion of Mesenchymal stem cells. GVHD is a pleiotropic disease involving any anatomical district; also, Ruxolitinib represents the standard for steroid-refractory cGVHD in this setting. It is a pleiotropic disease involving any anatomical district; also, Ruxolitinib represents the standard for steroid-refractory cGVHD in this setting. Extracorporeal Photopheresis (ECP) is still an option used for steroid refractoriness or to achieve a steroid-sparing. For Ruxolitinib-refractory cGVHD, Belumosudil and Axatilimab represent the most promising agents. Bronchiolitis obliterans syndrome (BOS) still represents a challenge; among the compounds targeting non-immune effectors, Alvelestat, a Neutrophil elastase inhibitor, seems promising in BOS. Finally, in both aGVHD and cGVHD, the association of biological markers with specific disease manifestations could help refine risk stratification and the availability of reliable biomarkers for specific treatments.
Keywords: graft versus host prophylaxis; graft versus host treatment; transplantation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Arai S., Arora M., Wang T., Spellman S.R., He W., Couriel D.R., Urbano-Ispizua A., Cutler C.S., Bacigalupo A.A., Battiwalla M., et al. Increasing incidence of chronic graft-versus-host disease in allogeneic transplantation: A report from the Center for International Blood and Marrow Transplant Research. Biol. Blood Marrow Transplant. 2015;21:266–274. doi: 10.1016/j.bbmt.2014.10.021. - DOI - PMC - PubMed
-
- Harris A.C., Young R., Devine S., Hogan W.J., Ayuk F., Bunworasate U., Chanswangphuwana C., Efebera Y.A., Holler E., Litzow M., et al. International, Multicenter Standardization of Acute Graft-versus-Host Disease Clinical Data Collection: A Report from the Mount Sinai Acute GVHD International Consortium. Biol. Blood Marrow Transplant. 2016;22:4–10. doi: 10.1016/j.bbmt.2015.09.001. - DOI - PMC - PubMed
-
- Filipovich A.H., Weisdorf D., Pavletic S., Socie G., Wingard J.R., Lee S.J., Martin P., Chien J., Przepiorka D., Couriel D., et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2005;11:945–956. doi: 10.1016/j.bbmt.2005.09.004. - DOI - PubMed
-
- Jagasia M.H., Greinix H.T., Arora M., Williams K.M., Wolff D., Cowen E.W., Palmer J., Weisdorf D., Treister N.S., Cheng G.-S., et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2015;21:389–401.e1. doi: 10.1016/j.bbmt.2014.12.001. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
