

The Effect of Exercise Training on Blood Lipids: A Systematic Review and Meta-analysis
- PMID: 39331324
- PMCID: PMC11787149
- DOI: 10.1007/s40279-024-02115-z
The Effect of Exercise Training on Blood Lipids: A Systematic Review and Meta-analysis
Abstract
Background: Dyslipidemia is a primary risk factor for cardiovascular disease (CVD). Exercise training (EXTr) improves some lipid markers but not others; the literature is dated and analyses may be underpowered.
Objectives: To clarify which lipid markers are altered with ExTr and establish if information size had yet reached futility.
Methods: We conducted a systematic review/meta-analysis, with meta-regression, to establish expected effect size in lipid profile with aerobic (AT), resistance (RT) and combined (CT = AT + RT) ExTr. We conducted trial sequence analysis (TSA) to control for type I and II error and establish if information size had reached futility.
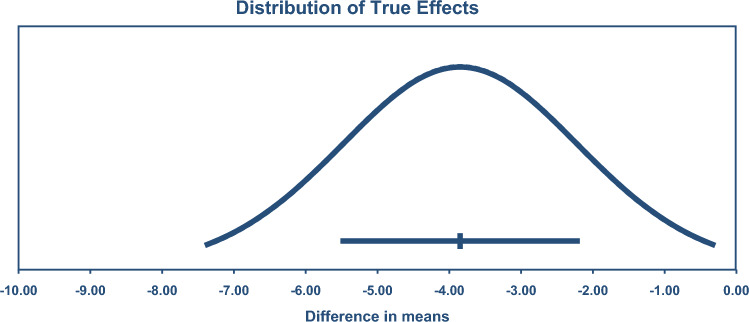
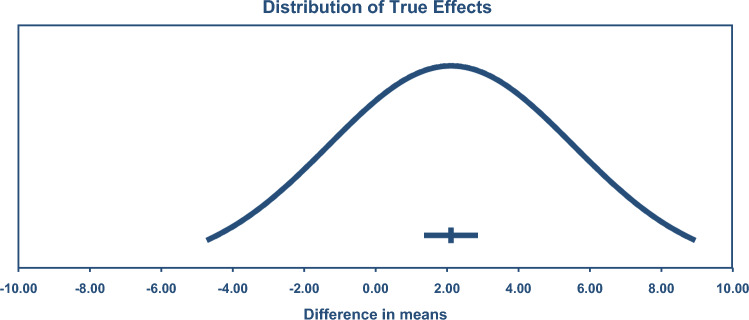
Results: We included 148 relevant randomized controlled trials (RCTs) of ExTr, with 227 intervention groups, total 8673 participants; exercise 5273, sedentary control 3400. Total cholesterol (TC) MD - 5.90 mg/dL (95% confidence interval (CI) - 8.14, - 3.65), high-density lipoprotein cholesterol (HDL) 2.11 (95% CI 1.43, 2.79), low-density lipoprotein cholesterol (LDL) - 7.22 (95% CI - 9.08, - 5.35), triglycerides - 8.01 (95% CI - 10.45, - 5.58) and very low-density lipoprotein cholesterol (VLDL) - 3.85 (95% CI - 5.49, - 2.22) all showed significant but modest 3.5-11.7%, improvements following ExTr. TSA indicated all analyses exceeded minimum information size to reach futility. CT was optimal for dyslipidemia management. Meta-regression showed every extra weekly aerobic session reduced TC - 7.68 mg/dL and for every extra week of training by - 0.5 mg/dL. Each minute of session time produced an additional 2.11 mg/dL HDL increase.
Conclusion: TSA analysis revealed sufficient data exist to confirm ExTr will improve all five lipid outcomes. CT is optimal for lipid management. The modest effect observed may moderate dyslipidemia medication for primary prevention. Prediction intervals suggest TC, HDL, LDL and TGD are only improved in one-quarter of studies.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Financial Support and Sponsorship: None. Conflicts of Interest: Nothing to report. Author Contributions: Neil Smart—Conceived the idea, refined the idea, extracted data, conducted data analysis, wrote the draft manuscript, assembled supplementary files. Corresponding author.D. Downes—Refined the idea, extracted data, conducted some data analysis, edited the draft paper. T. Van der Touw—Refined the idea, extracted data, conducted some data analysis, edited the draft paper, assembled some supplementary files.S. Hada—Refined the idea, extracted data, conducted some data analysis, provided minor edits of the draft paper. G. Dieberg—Refined the idea, extracted data, conducted some data analysis, edited the draft manuscript, assembled some supplementary files. M.J. Pearson—Refined the idea, extracted data, conducted some data analysis, edited the draft manuscript, assembled some supplementary files. M. Wolden—Refined the idea, extracted data, conducted data analysis, edited the draft manuscript, assembled some supplementary files. N. King—Refined the idea, extracted data, conducted some data analysis, edited the draft manuscript, assembled some supplementary files.S.P.J. Goodman—Refined the idea, extracted data, conducted some data analysis and risk of bias analysis, edited the draft manuscript, assembled some supplementary files. All authors read and approved the final version of the manuscript.
Figures





References
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082–143. - PMC - PubMed
-
- Barkas F, Milionis H, Kostapanos MS, Mikhailidis DP, Elisaf M, Liberopoulos E. How effective are the ESC/EAS and 2013 ACC/AHA guidelines in treating dyslipidemia? Lessons from a lipid clinic. Curr Med Res Opin. 2015;31(2):221–8. - PubMed
-
- Kraus WE, Houmard JA, Duscha BD, Knetzger KJ, Wharton MB, McCartney JS, et al. Effects of the amount and intensity of exercise on plasma lipoproteins. N Engl J Med. 2002;347(19):1483–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
