

Glucagon-Producing Pancreatic Neuroendocrine Tumors (Glucagonomas) are Enriched in Aggressive Neoplasms with ARX and PDX1 Co-expression, DAXX/ATRX Mutations, and ALT (Alternative Lengthening of Telomeres)
- PMID: 39331358
- PMCID: PMC11659356
- DOI: 10.1007/s12022-024-09826-z
Glucagon-Producing Pancreatic Neuroendocrine Tumors (Glucagonomas) are Enriched in Aggressive Neoplasms with ARX and PDX1 Co-expression, DAXX/ATRX Mutations, and ALT (Alternative Lengthening of Telomeres)
Abstract
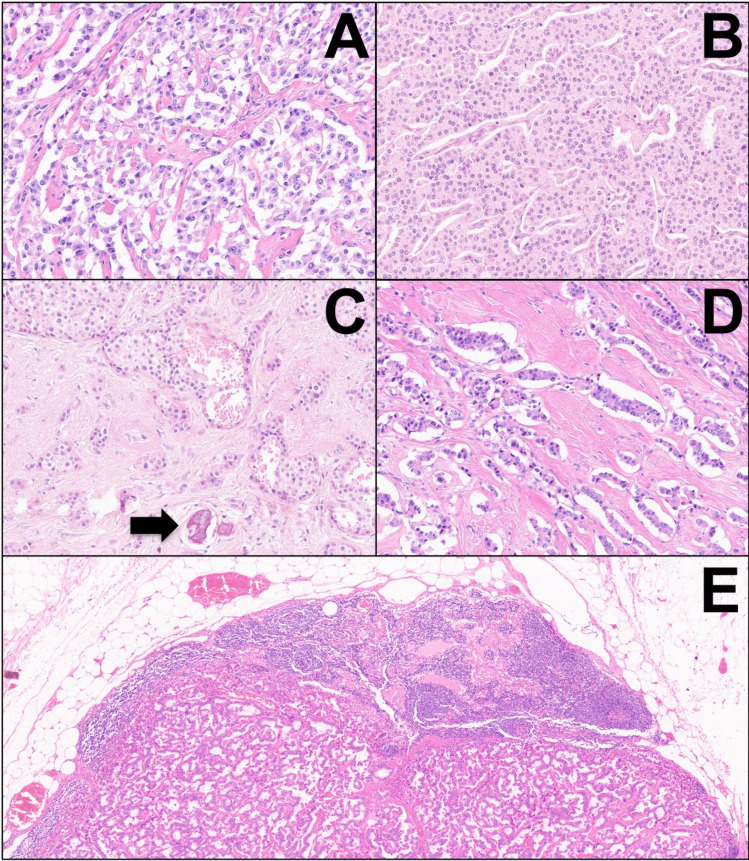
Glucagonomas are functioning pancreatic neuroendocrine tumors (PanNETs) responsible for glucagonoma syndrome. This study aims to shed light on the clinicopathological and molecular features of these neoplasms. Six patients with glucagonomas were identified. All neoplasms were investigated with immunohistochemistry for neuroendocrine markers (Synaptophysin, Chromogranin-A), ATRX, DAXX, ARX, and PDX1 transcription factors. Fluorescent in situ hybridization (FISH) for assessing alternative lengthening of telomeres (ALT), and next-generation sequencing (NGS) for molecular profiling were performed. All cases were large single masses (mean size of 8.2 cm), with necrolytic migratory erythema as the most common symptom (6/6 cases, 100%). All neoplasms were well-differentiated G1 tumors, except one case that was G2. The tumors consistently showed classic/conventional histomorphology, with solid-trabecular and nested architecture. Lymphatic and vascular invasion (6/6, 100%), perineural infiltration (4/6, 66.6%), and nodal metastasis (4/6, 66.6%) were frequently observed. Transcription factors expression showed strong ARX expression in all tumors, and PDX1 expression in 5/6 cases (83.3%), indicating co-occurring alpha- and beta-cell differentiation. NGS showed recurrent somatic MEN1 and ATRX/DAXX biallelic inactivation. Cases with ATRX or DAXX mutations also showed matched loss of ATRX or DAXX protein expression and ALT. One case harbored somatic MUTYH inactivation and showed a high tumor mutational burden (TMB, 41.0 mut/Mb). During follow-up, one patient died of the disease, and four patients developed distant metastasis. Pancreatic glucagonomas are distinct PanNETs with specific clinicopathological and molecular features, including histological aspects of biological aggressiveness, co-occurring alpha- and beta-cell differentiation, MEN1 and DAXX/ATRX mutations enrichment, and the possible presence of high-TMB as an actionable marker.
Keywords: ALT; ATRX; DAXX; Functioning; Glucagon; MUTYH; NET; Neuroendocrine.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing Interests: The authors declare no competing interests.
Figures

References
-
- Rindi G, Mete O, Uccella S, Basturk O, La Rosa S, Brosens LAA, Ezzat S, de Herder WW, Klimstra DS, Papotti M, Asa SL (2022). Overview of the 2022 WHO Classification of Neuroendocrine Neoplasms. Endocr Pathol 33(1):115-154. 10.1007/s12022-022-09708-2 - PubMed
-
- Massironi S (2024). The diagnostic challenges of functioning neuroendocrine tumors: balancing accuracy, availability, and personalized care. Expert Rev Endocrinol Metab 19(2):99-101. 10.1080/17446651.2024.2320639 - PubMed
-
- Hofland J, Falconi M, Christ E, Castaño JP, Faggiano A, Lamarca A, Perren A, Petrucci S, Prasad Vikas, Rusznieski P, Thirlwell C, Vullierme M, Welin S, Bartsch D (2023). European Neuroendocrine Tumor Society 2023 guidance paper for functioning pancreatic neuroendocrine tumour syndromes. J Neuroendocrinol 35(8):e13318. https://doi.org/:10.1111/jne.13318 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
