

Enhancing aesthetic outcomes: The role of biomechanics in periorbital and eyelid cosmetic surgery
- PMID: 39331432
- PMCID: PMC11573038
- DOI: 10.4103/IJO.IJO_1549_23
Enhancing aesthetic outcomes: The role of biomechanics in periorbital and eyelid cosmetic surgery
Abstract
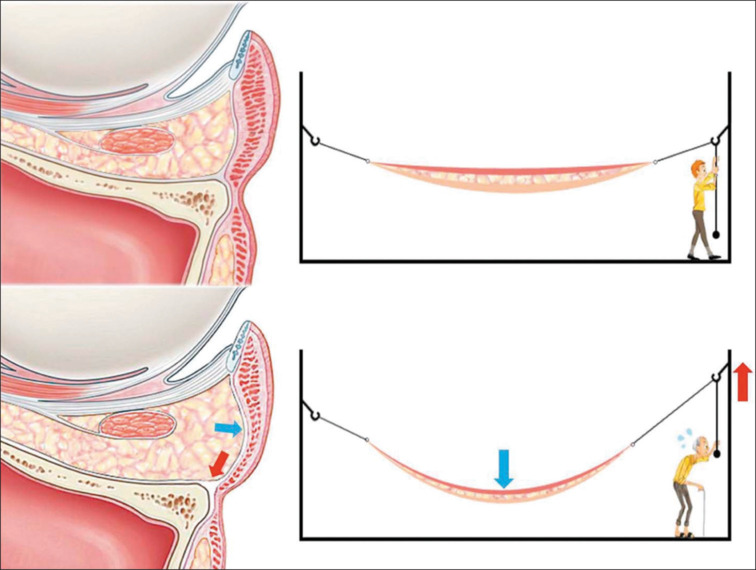
Cosmetic periorbital and eyelid surgery is a commonly performed procedure in facial plastic surgery. Understanding the biomechanics of periorbital anatomy and its role in aesthetic surgery is essential for achieving optimal outcomes. This review explores the biomechanical processes involved in periorbital age changes and analyzes the impact of cosmetic surgery approaches on these processes. By maintaining the initial mechanical equilibrium of the brows, eyelids, septal fat, and blepharoplasty folds, periorbital and eyelid cosmetic surgery can effectively rejuvenate the appearance. Disruption of this equilibrium can lead to the migration of anatomic components, resulting in signs of aging. Surgeons, by applying biomechanical concepts, can tailor the forces exerted upon the different structures to manifest the patient's aesthetic aspirations. The key to success in periorbital and eyelid cosmetic surgery lies in re-establishing a dynamic mechanical equilibrium within the periorbital framework.
Copyright © 2024 Copyright: © 2024 Indian Journal of Ophthalmology.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Ksander GA, Vistnes LM, Rose EH. Excisional wound biomechanics, skin tension lines, and elastic contraction. Plast Reconstr Surg. 1977;59:398–406. - PubMed
-
- Fernandes MG, da Silva LP, Cerqueira MT, Ibañez R, Murphy CM, Reis RL, et al. Mechanomodulatory biomaterials prospects in scar prevention and treatment. Acta Biomater. 2022;150:22–33. - PubMed
-
- Furnas DW, Fischer GW. The Z-plasty: Biomechanics and mathematics. Br J Plast Surg. 1971;24:144–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
