

Daratumumab with lenalidomide as maintenance after transplant in newly diagnosed multiple myeloma: the AURIGA study
- PMID: 39331724
- PMCID: PMC11775507
- DOI: 10.1182/blood.2024025746
Daratumumab with lenalidomide as maintenance after transplant in newly diagnosed multiple myeloma: the AURIGA study
Abstract
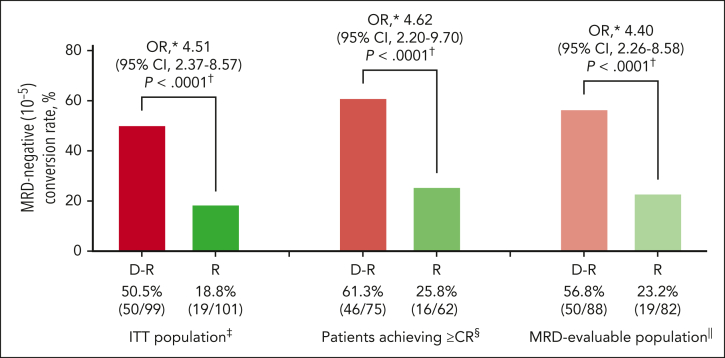
No randomized trial has directly compared daratumumab and lenalidomide (D-R) maintenance with standard-of-care lenalidomide (R) alone after transplant. Herein, we report the primary results of the phase 3 AURIGA study evaluating D-R vs R maintenance in patients with newly diagnosed multiple myeloma (NDMM) who had very good or better partial response, were minimal residual disease (MRD)-positive (10-5) and anti-CD38-naïve after transplant. Two hundred patients were randomly assigned (1:1) to D-R (n = 99) or R (n = 101) maintenance for up to 36 cycles. The MRD-negative (10-5) conversion rate by 12 months from start of maintenance (primary end point) was significantly higher for D-R than R (50.5% vs 18.8%; odds ratio [OR], 4.51; 95% confidence interval [CI], 2.37-8.57; P < .0001). MRD-negative (10-6) conversion rate was similarly higher with D-R (23.2% vs 5.0%; OR, 5.97; 95% CI, 2.15-16.58; P = .0002). At median follow-up (32.3 months), D-R achieved a higher overall MRD-negative (10-5) conversion rate (D-R, 60.6% vs R, 27.7%; OR, 4.12; 95% CI, 2.26-7.52; P < .0001) and complete response rate or better (75.8% vs 61.4%; OR, 2.00; 95% CI, 1.08-3.69; P = .0255) vs R. Progression-free survival (PFS) favored D-R vs R (hazard ratio, 0.53; 95% CI, 0.29-0.97); estimated 30-month PFS rates were 82.7% for D-R and 66.4% for R. Incidences of grade 3/4 cytopenias (54.2% vs 46.9%) and infections (18.8% vs 13.3%) were slightly higher with D-R than R. In conclusion, D-R maintenance achieved a higher MRD-negative conversion rate and improved PFS after transplant vs R, with no new safety concerns. This trial was registered at www.clinicaltrials.gov as #NCT03901963.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: A.B. received research funding from Bristol Myers Squibb (BMS), GSK, BeiGene, Roche, and Janssen. L.F. served on advisory boards and as a site principal investigator for BMS and Janssen Biotech Inc. L.D.A. served as a consultant and on advisory boards for Janssen, Celgene, BMS, Amgen, GSK, AbbVie, BeiGene, Cellectar, Sanofi, and Prothena and served on the data safety monitoring board for Prothena. C.P.C. received honoraria from Janssen and Sanofi Genzyme. A.J.C. served as a consultant or in an advisory role for Sebia, Janssen, BMS, Sanofi, HopeAI, Adaptive Biotechnologies, and AbbVie and received research funding from Janssen, BMS, Juno/Celgene, Sanofi, Regeneron, IGM Biosciences, Nektar, Harpoon, and Caelum. C.C. served as a consultant for BMS, Janssen, Pfizer, Karyopharm, and Genentech and received research funding from BMS, Janssen, Takeda, Ionis, Poseida, and Harpoon. S.L. received research funding from Janssen, Allogene (Inst), Bioline (Inst), Pfizer (Inst), BMS (Inst), Regeneron (Inst), Sanofi (Inst), Ionis (Inst), and ImmPACT Bio (Inst) and owns stock or stock options for TORL Biotherapeutics. D.W.S. served as a consultant or in an advisory role for GSK, Janssen, Sanofi, AbbVie, BMS, Pfizer, Arcellx, Bioline, AstraZeneca, and Genentech and received research funding from Pfizer. K.H.S. served on an advisory board for Janssen, Sanofi, and GSK; received research funding from AbbVie and Karyopharm; and received honoraria from Karyopharm, Janssen, Adaptive Biotechnologies, GSK, BMS, Sanofi Genzyme, and Regeneron. R.S. served as a consultant or in an advisory role for Sanofi-Aventis, Janssen Oncology, and Oncopeptides and received research funding from Sanofi. N.S. is a current employee and stockholder of AstraZeneca. A. Chung served as a consultant and on an advisory board for Janssen and received research funding from AbbVie, BMS, Caelum, CARsgen, Cellectis, Janssen, K36 Therapeutics, and Merck. M.K., H.P., S.P., V.K., A. Cortoos, R.C., and T.S.L. are employees of Janssen (Johnson & Johnson) and may hold stock. P.V. served as a consultant for, received honoraria from, and holds a membership on the board of directors or advisory committees for AbbVie, BMS, Karyopharm, Regeneron, and Sanofi. E.P. declares no competing financial interests.
Figures




References
-
- Goicoechea I, Puig N, Cedena MT, et al. Deep MRD profiling defines outcome and unveils different modes of treatment resistance in standard- and high-risk myeloma. Blood. 2021;137(1):49–60. - PubMed
-
- International Myeloma Foundation A historic turning point: ODAC unanimously votes in favor of MRD testing as an early endpoint in myeloma clinical trials to support accelerated approvals of new treatments. https://www.myeloma.org/blog/dr-duries/odac-unanimously-in-favor-mrd-tes...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
