

Cytokine-mediated CAR T therapy resistance in AML
- PMID: 39333315
- PMCID: PMC12118809
- DOI: 10.1038/s41591-024-03271-5
Cytokine-mediated CAR T therapy resistance in AML
Abstract
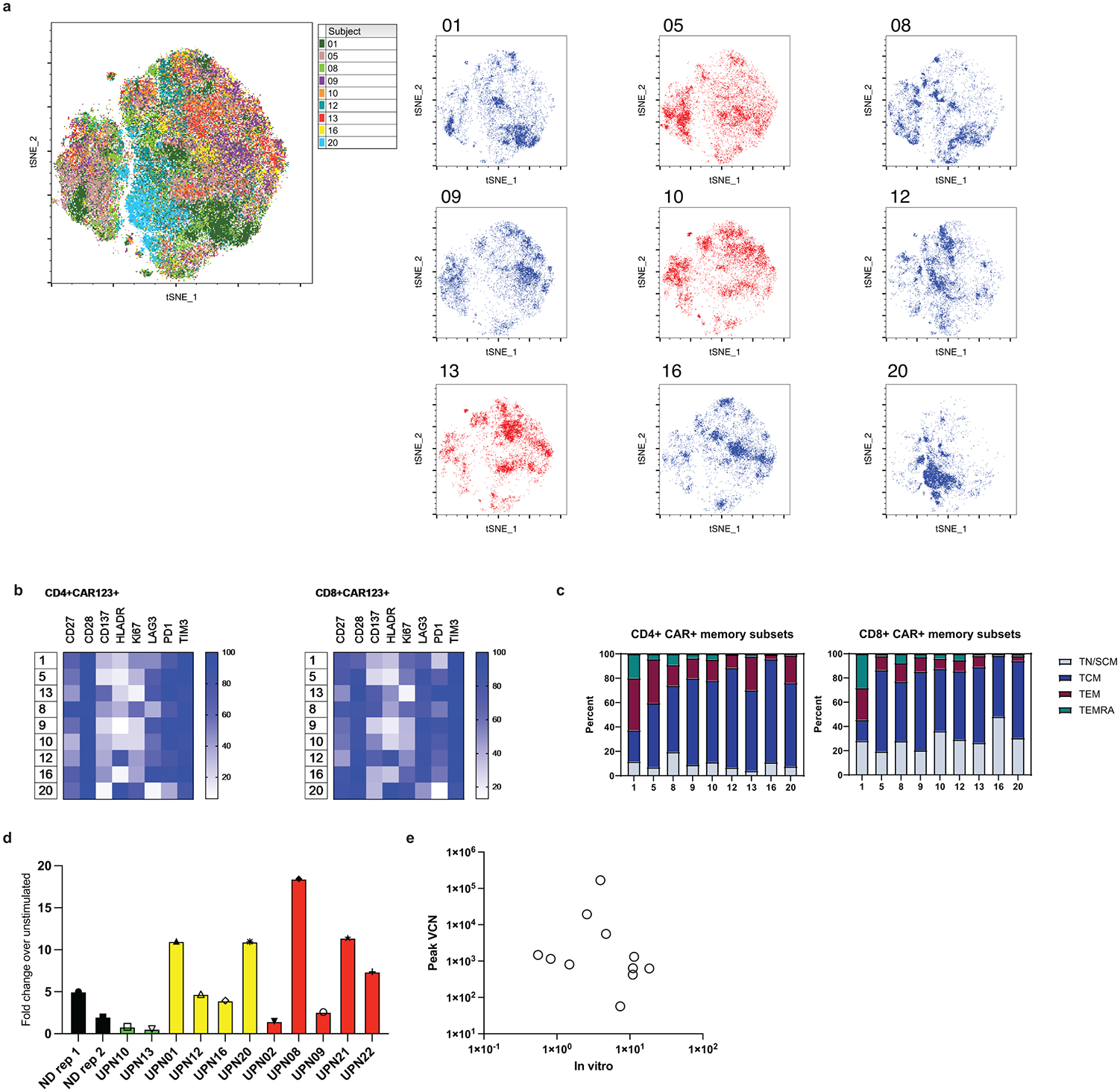
Acute myeloid leukemia (AML) is a rapidly progressive malignancy without effective therapies for refractory disease. So far, chimeric antigen receptor (CAR) T cell therapy in AML has not recapitulated the efficacy seen in B cell malignancies. Here we report a pilot study of autologous anti-CD123 CAR T cells in 12 adults with relapsed or refractory AML. CAR T cells targeting CD123+ cells were successfully manufactured in 90.4% of runs. Cytokine release syndrome was observed in 10 of 12 infused individuals (83.3%, 90% confidence interval 0.5-0.97). Three individuals achieved clinical response (25%, 90% confidence interval 0.07-0.53). We found that myeloid-supporting cytokines are secreted during cell therapy and support AML blast survival via kinase signaling, leading to CAR T cell exhaustion. The prosurvival effect of therapy-induced cytokines presents a unique resistance mechanism in AML that is distinct from any observed in B cell malignancies. Our findings suggest that autologous CART manufacturing is feasible in AML, but treatment is associated with high rates of cytokine release syndrome and relatively poor clinical efficacy. Combining CAR T cell therapies with cytokine signaling inhibitors could enhance immunotherapy efficacy in AML and achieve improved outcomes (ClinicalTrials.gov identifier: NCT03766126 ).
© 2024. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing interests: D.L.P. declares funding from the National Marrow Donor Program; membership on an entity’s Board of Directors or advisory committees of Kite/Gilead, Janssen, Genentech, DeCart, Sana Biotechnology, Verismo and Novartis; is a current equity holder of the American Society for Transplantation and Cellular Therapy and Verismo; declares honoraria for Incyte; and has patents and royalties in Tmunity and Wiley and Sons Publishing. J.A.F. is a member of the scientific advisory boards of Cartography Bio and Shennon Biotechnologies and has patents, royalties and other intellectual property. M.R.L. is an employee of Hematoloics, Inc. J.L.B. is an employee of Novartis. C.H.J. is an inventor of patents related to CAR therapy products and may be eligible to receive a select portion of royalties paid from Kite to the University of Pennsylvania. C.H.J. is a scientific cofounder and holds equity in Capstan Therapeutics, Dispatch Biotherapeutics and Bluewhale Bio. C.H.J. serves on the board of AC Immune and is a scientific advisor to BlueSphere Bio, Cabaletta, Carisma, Cartography, Cellares, Cellcarta, Celldex, Danaher, Decheng, ImmuneSensor, Kite, Poseida, Verismo, Viracta and WIRB-Copernicus group. S.I.G. has patents related to CAR therapy with royalties paid from Novartis to the University of Pennsylvania. S.I.G. is a scientific cofounder and holds equity in Interius Biotherapeutics and Carisma Therapeutics. S.I.G. is a scientific advisor to Carisma, Cartography, Currus, Interius, Kite, NKILT and Mission Bio. The other authors declare no competing interests.
Figures








References
-
- Kantarjian H. Acute myeloid leukemia--major progress over four decades and glimpses into the future. Am J Hematol. 2016;91(1):131–45. - PubMed
-
- Perl AE, Martinelli G, Cortes JE, Neubauer A, Berman E, Paolini S, et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3-Mutated AML. N Engl J Med. 2019;381(18):1728–40. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- 5T32HD043021/U.S. Department of Health & Human Services | NIH | Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD)
- P01CA214278-05/U.S. Department of Health & Human Services | NIH | National Cancer Institute (NCI)
- T32 HD043021/HD/NICHD NIH HHS/United States
- P01 CA214278/CA/NCI NIH HHS/United States
- 2023-0221/Doris Duke Charitable Foundation (DDCF)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
