

Blood-based DNA methylation and exposure risk scores predict PTSD with high accuracy in military and civilian cohorts
- PMID: 39334086
- PMCID: PMC11429352
- DOI: 10.1186/s12920-024-02002-6
Blood-based DNA methylation and exposure risk scores predict PTSD with high accuracy in military and civilian cohorts
Abstract
Background: Incorporating genomic data into risk prediction has become an increasingly popular approach for rapid identification of individuals most at risk for complex disorders such as PTSD. Our goal was to develop and validate Methylation Risk Scores (MRS) using machine learning to distinguish individuals who have PTSD from those who do not.
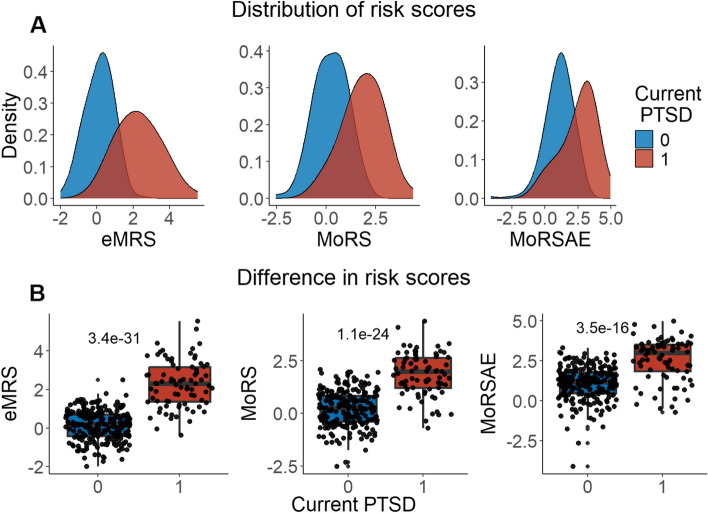
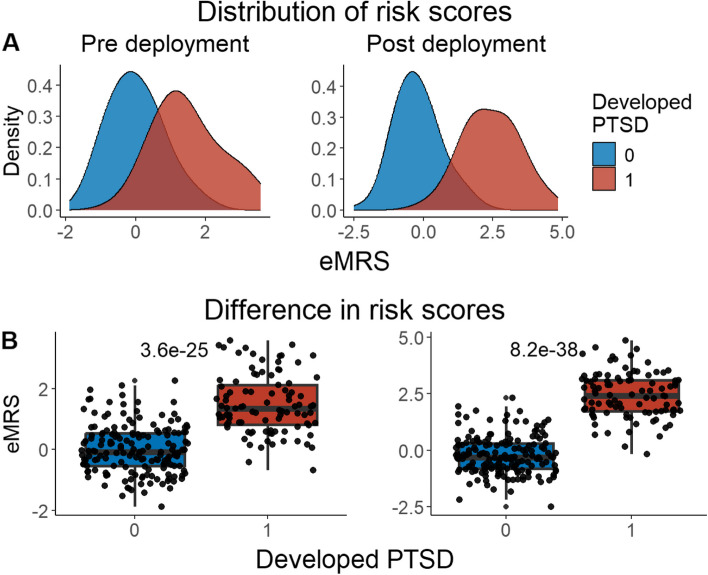
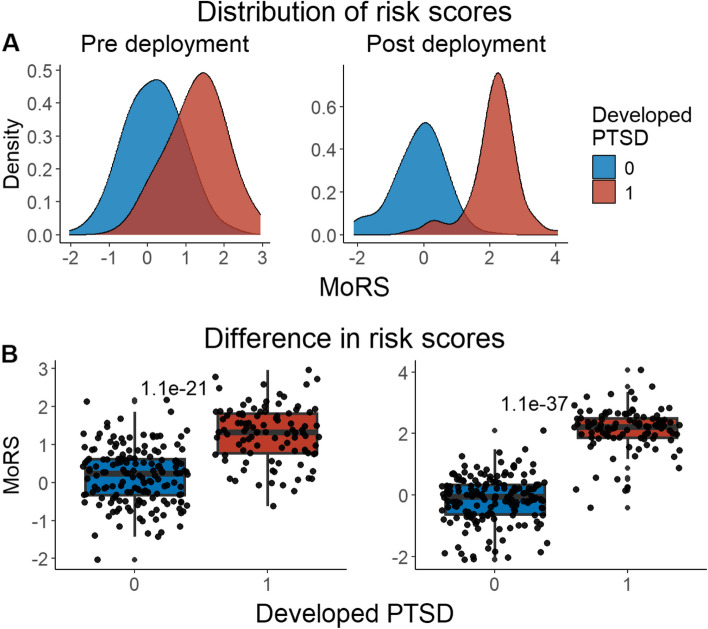
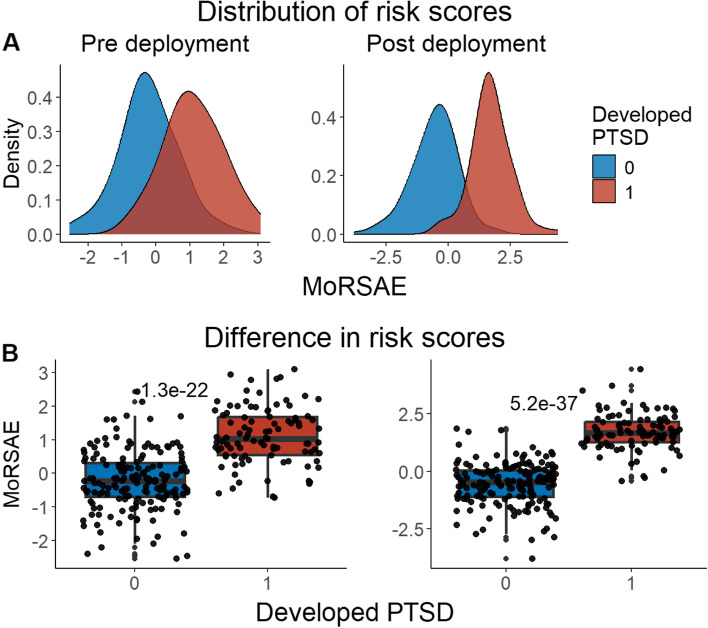
Methods: Elastic Net was used to develop three risk score models using a discovery dataset (n = 1226; 314 cases, 912 controls) comprised of 5 diverse cohorts with available blood-derived DNA methylation (DNAm) measured on the Illumina Epic BeadChip. The first risk score, exposure and methylation risk score (eMRS) used cumulative and childhood trauma exposure and DNAm variables; the second, methylation-only risk score (MoRS) was based solely on DNAm data; the third, methylation-only risk scores with adjusted exposure variables (MoRSAE) utilized DNAm data adjusted for the two exposure variables. The potential of these risk scores to predict future PTSD based on pre-deployment data was also assessed. External validation of risk scores was conducted in four independent cohorts.
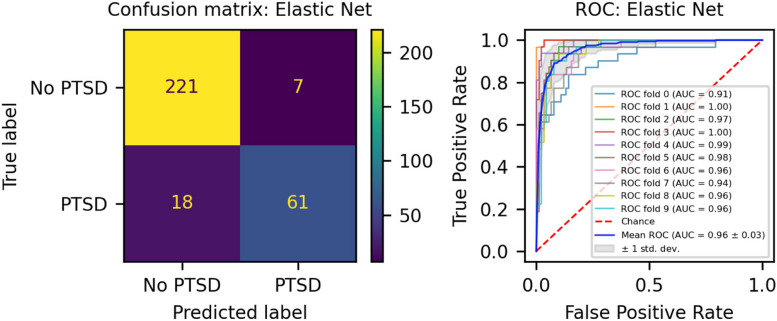
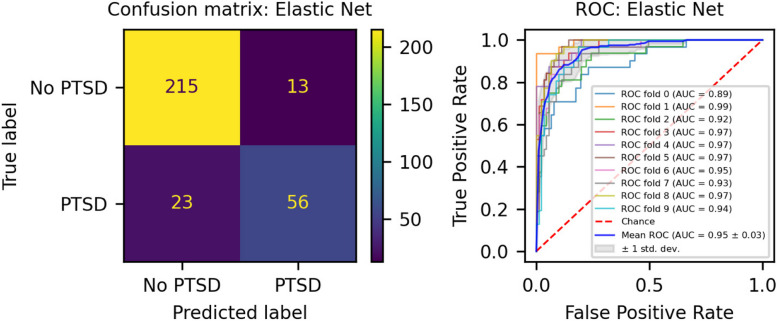
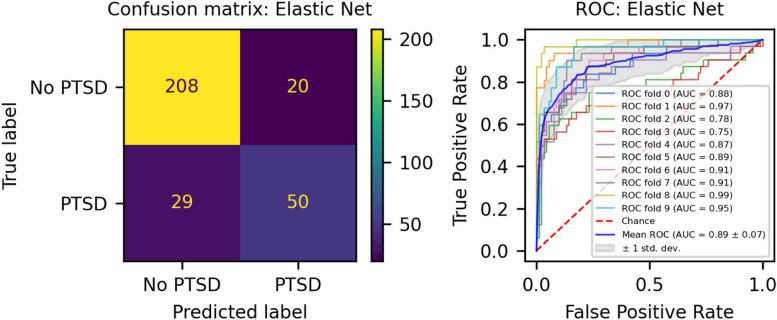
Results: The eMRS model showed the highest accuracy (92%), precision (91%), recall (87%), and f1-score (89%) in classifying PTSD using 3730 features. While still highly accurate, the MoRS (accuracy = 89%) using 3728 features and MoRSAE (accuracy = 84%) using 4150 features showed a decline in classification power. eMRS significantly predicted PTSD in one of the four independent cohorts, the BEAR cohort (beta = 0.6839, p=0.006), but not in the remaining three cohorts. Pre-deployment risk scores from all models (eMRS, beta = 1.92; MoRS, beta = 1.99 and MoRSAE, beta = 1.77) displayed a significant (p < 0.001) predictive power for post-deployment PTSD.
Conclusion: The inclusion of exposure variables adds to the predictive power of MRS. Classification-based MRS may be useful in predicting risk of future PTSD in populations with anticipated trauma exposure. As more data become available, including additional molecular, environmental, and psychosocial factors in these scores may enhance their accuracy in predicting PTSD and, relatedly, improve their performance in independent cohorts.
Keywords: DNA methylation; Machine learning; PTSD; Risk scores.
© 2024. The Author(s).
Conflict of interest statement
Murray B. Stein has in the past 3 years received consulting income from Acadia Pharmaceuticals, Aptinyx, atai Life Sciences, BigHealth, Biogen, Bionomics, BioXcel Therapeutics, Boehringer Ingelheim, Clexio, Delix Therapeutics, Eisai, EmpowerPharm, Engrail Therapeutics, Janssen, Jazz Pharmaceuticals, NeuroTrauma Sciences, PureTech Health, Sage Therapeutics, Sumitomo Pharma, and Roche/Genentech. Dr. Stein has stock options in Oxeia Biopharmaceuticals and EpiVario. He has been paid for his editorial work on Depression and Anxiety (Editor-in-Chief), Biological Psychiatry (Deputy Editor), and UpToDate (Co-Editor-in-Chief for Psychiatry). He has also received research support from NIH, Department of Veterans Affairs, and the Department of Defense. He is on the scientific advisory board for the Brain and Behavior Research Foundation and the Anxiety and Depression Association of America. Dr. Chia-Yen Chen is an employee of Biogen. Dr. Nikolaos P. Daskalakis has served on scientific advisory boards for BioVie Pharma, Circular Genomics and Sentio Solutions for unrelated work. Dr. Nicole R. Nugent is a member of the scientific advisory board for Ilumivu. Dr. Sheila Rauch support from Wounded Warrior Project (WWP), Department of Veterans Affairs (VA), National Institute of Health (NIH), McCormick Foundation, Tonix Pharmaceuticals, Woodruff Foundation, and Department of Defense (DOD). Dr. Rauch also receives royalties from Oxford University Press and American Psychological Association Press. Dr Ressler reported receiving personal consulting fees from Sage Therapeutics, Senseye, Boerhinger Ingelheim, Jazz Pharmaceuticals, and Acer, Inc. and a sponsored research grant from Alto Neuroscience outside the submitted work.
Figures
Update of
-
Blood-based DNA methylation and exposure risk scores predict PTSD with high accuracy in military and civilian cohorts.Res Sq [Preprint]. 2024 Feb 15:rs.3.rs-3952163. doi: 10.21203/rs.3.rs-3952163/v1. Res Sq. 2024. Update in: BMC Med Genomics. 2024 Sep 27;17(1):235. doi: 10.1186/s12920-024-02002-6. PMID: 38410438 Free PMC article. Updated. Preprint.
References
-
- Kulka RA, Schlenger WE, Fairbank JA, Hough RL, Jordan BK, Marmar CR, et al. Trauma and the Vietnam war generation: Report of findings from the National Vietnam Veterans Readjustment Study. Philadelphia: Brunner/Mazel; 1990. xxix, 322-xxix, p.
-
- Brady KT, Killeen TK, Brewerton T, Lucerini S. Comorbidity of psychiatric disorders and posttraumatic stress disorder. J Clin Psychiatry. 2000;61(Suppl 7):22–32. - PubMed
MeSH terms
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- R01MH106595/NH/NIH HHS/United States
- B3001-C/VA Rehabilitation Research and Development Traumatic Brain Injury National Research Center
- 917.18.336/The Dutch Research Council
- #W81XWH-11-1-0073/U.S. Department of Defense
- R01MD011728/National Institutes for Minority Health and Health Disparities
- BX005872/U.S. Department of Veterans Affairs
- IK2 CX002343/CX/CSRD VA/United States
- I01 CX-001276-01/U.S. Department of Veterans Affairs
- RF1 AG068121/AG/NIA NIH HHS/United States
- R01MH108826/The National Institute of Mental Health
- K23MH112852/MH/NIMH NIH HHS/United States
- OPP 1017641/Bill and Melinda Gates Foundation
- I21 BX005872/BX/BLRD VA/United States
- R01 MH105379/MH/NIMH NIH HHS/United States
- I01 CX001276/CX/CSRD VA/United States
- R01 MH106595/MH/NIMH NIH HHS/United States
- K23 MH112852/MH/NIMH NIH HHS/United States
- R01MH105379/MH/NIMH NIH HHS/United States
- R01 MD011728/MD/NIMHD NIH HHS/United States
- U01 MH087981/MH/NIMH NIH HHS/United States
- K12 HD085850/HD/NICHD NIH HHS/United States
- K12HD085850/National Institutes of Health, United States
- R01 MH108826/MH/NIMH NIH HHS/United States
- UL1TR000433/TR/NCATS NIH HHS/United States
- U01MH087981/MH/NIMH NIH HHS/United States
- RF1AG068121/The National Institute of Aging, United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
