

Telehealth exercise for continence after gynaecological cancer treatment (TELE-CONNECT): a protocol for a co-designed pragmatic randomised controlled trial
- PMID: 39334122
- PMCID: PMC11430120
- DOI: 10.1186/s12905-024-03365-9
Telehealth exercise for continence after gynaecological cancer treatment (TELE-CONNECT): a protocol for a co-designed pragmatic randomised controlled trial
Abstract
Background: Urinary incontinence (UI) is the most prevalent pelvic floor disorder following treatment for gynaecological cancer with a distressing impact on quality-of-life in survivors. Physiotherapist-supervised pelvic floor muscle (PFM) training is recommended as the first-line intervention for UI in community-dwelling women. However, it is not known if this intervention is effective in women following treatment for gynaecological cancer, nor whether PFM training can be delivered entirely remotely. The primary aim of this study is to investigate if a telehealth-delivered PFM training program incorporating a novel biofeedback device reduces UI compared with usual care, following gynaecological cancer.
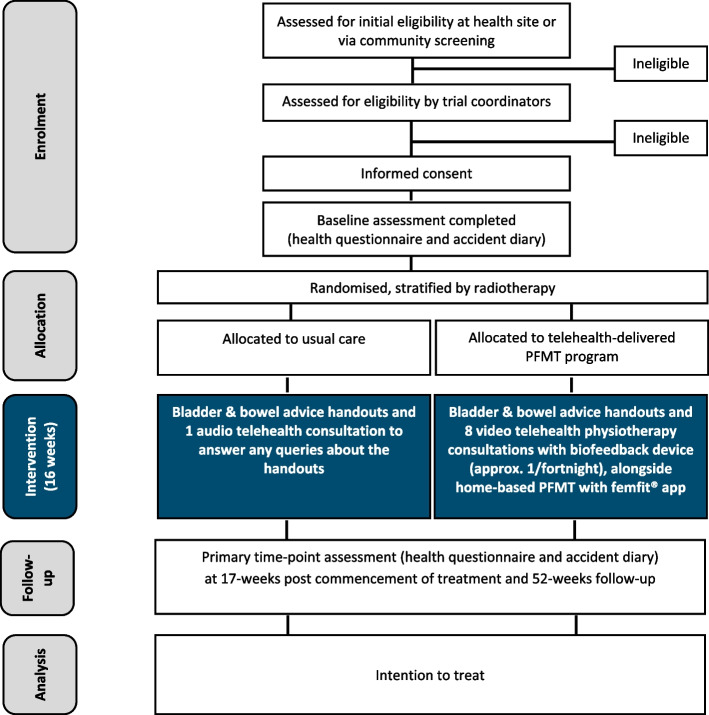
Methods: This is a pragmatic, two-arm parallel-group, stratified superiority randomised controlled trial recruiting 72 participants (ACTRN12622000580774). Recruitment sites include gynaecology-oncology outpatient clinics, supplemented by advertisements through community foundations/social media/care groups. Participants must have completed primary cancer treatment at least 6 months prior or adjuvant therapy at least 3 months prior, for Stage I, II or III uterine, cervical, fallopian tube, primary peritoneal or ovarian cancer or borderline ovarian tumour, and have UI occurring at least weekly. Participants randomised to the usual care group will receive bladder and bowel advice handouts and one audio telehealth physiotherapist consultation to answer any queries about the handouts. Participants randomised to the intervention group will receive the same handouts plus eight video telehealth physiotherapist consultations for PFM training with a biofeedback device (femfit®), alongside a home-based program over 16 weeks. The primary outcome measure is a patient-reported outcome of UI frequency, amount and interference with everyday life (measured using the International Consultation on Incontinence Questionnaire - Urinary Incontinence Short Form), immediately post-intervention compared with baseline. Secondary outcomes include quality-of-life measures, bother of pelvic floor symptoms, leakage episodes, use of continence pads and global impression of change. We will also investigate if the intervention improves intra-vaginal resting and squeeze pressure in women in the intervention arm, using data from the biofeedback device.
Discussion: If clinical effectiveness of telehealth-delivered physiotherapist-supervised PFM training, supplemented with home biofeedback is shown, this will allow this therapy to enter pathways of care, and provide an evidence-based option for treatment of post-cancer UI not currently available.
Trial registration: Australian New Zealand Clinical Trials Registry (ANZCTR), ID 12622000580774. Registered 20 April 2022.
Keywords: Biofeedback; Gynaecological cancer; Pelvic floor muscle training; Physiotherapy; Randomised controlled trial; Telehealth; Urinary incontinence.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Milsom I, Altman D, Cartwright R, Lapitan MC, Nelson R, Sjostrom S, et al. Epidemiology of urinary incontinence (UI) and and other lower urinary tract symtpoms (LUTS), pelvic organ prolapse (POP) and anal incontinence (AI). In: Cardozo LD, Rovner ES, Wagg A, Wein A, Abrams P, editors. 7th International Consultation. on Incontinence: Bristol: ICUD ICS; 2023. p. 13–130.
-
- Continence Fondation of Australia. Continence in Australia a snapshot June 2019. https://www.continence.org.au/news/2019-continence-in-australia-snapshot....
-
- Abrams P, Smith AP, Cotterill N. The impact of urinary incontinence on health-related quality of life (HRQoL) in a real-world population of women aged 45–60 years: results from a survey in France, Germany, the UK and the USA. BJU Int. 2015;115(1):143–52. - PubMed
-
- Brennen R, Lin KY, Denehy L, Soh SE, Jobling T, McNally OM et al. Natural history of pelvic floor disorders before and after hysterectomy for gynaecological cancer. BJOG. 2024. 10.1111/1471-0528.17870. Online ahead of print. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
