

Health workforce needs in Malawi: analysis of the Thanzi La Onse integrated epidemiological model of care
- PMID: 39334127
- PMCID: PMC11437829
- DOI: 10.1186/s12960-024-00949-2
Health workforce needs in Malawi: analysis of the Thanzi La Onse integrated epidemiological model of care
Abstract
Background: To make the best use of health resources, it is crucial to understand the healthcare needs of a population-including how needs will evolve and respond to changing epidemiological context and patient behaviour-and how this compares to the capabilities to deliver healthcare with the existing workforce. Existing approaches to planning either rely on using observed healthcare demand from a fixed historical period or using models to estimate healthcare needs within a narrow domain (e.g., a specific disease area or health programme). A new data-grounded modelling method is proposed by which healthcare needs and the capabilities of the healthcare workforce can be compared and analysed under a range of scenarios: in particular, when there is much greater propensity for healthcare seeking.
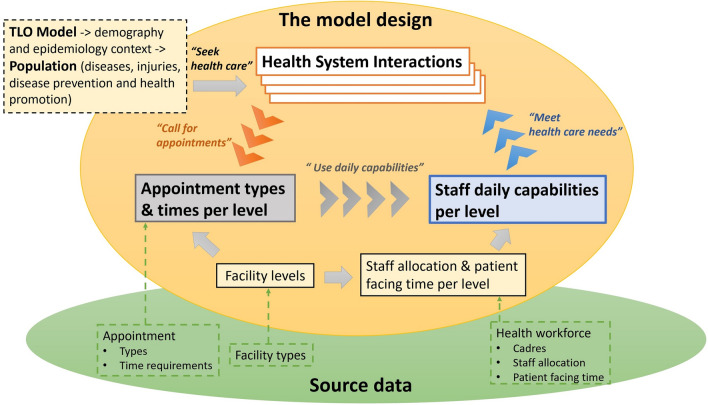
Methods: A model representation of the healthcare workforce, one that formalises how the time of the different cadres is drawn into the provision of units of healthcare, was integrated with an individual-based epidemiological model-the Thanzi La Onse model-that represents mechanistically the development of disease and ill-health and patients' healthcare seeking behaviour. The model was applied in Malawi using routinely available data and the estimates of the volume of health service delivered were tested against officially recorded data. Model estimates of the "time needed" and "time available" for each cadre were compared under different assumptions for whether vacant (or established) posts are filled and healthcare seeking behaviour.
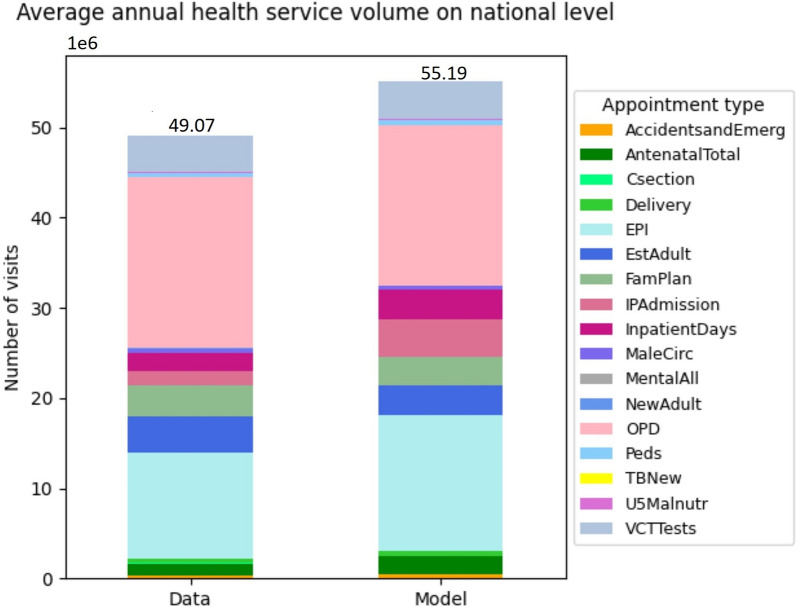
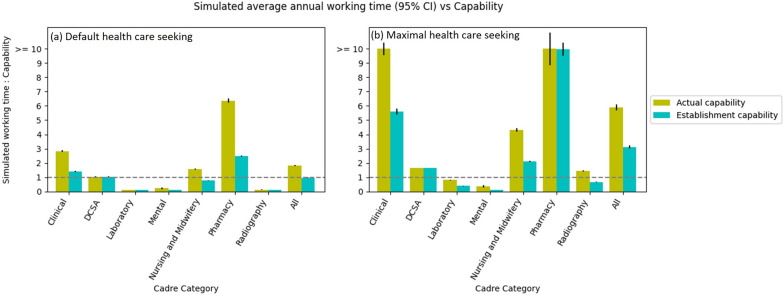
Results: The model estimates of volume of each type of service delivered were in good agreement with the available data. The "time needed" for the healthcare workforce greatly exceeded the "time available" (overall by 1.82-fold), especially for pharmacists (6.37-fold) and clinicians (2.83-fold). This discrepancy would be largely mitigated if all vacant posts were filled, but the large discrepancy would remain for pharmacists (2.49-fold). However, if all of those becoming ill did seek care immediately, the "time needed" would increase dramatically and exceed "time supply" (2.11-fold for nurses and midwives, 5.60-fold for clinicians, 9.98-fold for pharmacists) even when there were no vacant positions.
Conclusions: The results suggest that services are being delivered in less time on average than they should be, or that healthcare workers are working more time than contracted, or a combination of the two. Moreover, the analysis shows that the healthcare system could become overwhelmed if patients were more likely to seek care. It is not yet known what the health consequences of such changes would be but this new model provides-for the first time-a means to examine such questions.
Keywords: Health care needs; Health services; Health system interactions; Healthcare workforce; Model design.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Government of Malawi. Malawi human resources for health strategic plan 2018–2022. New Delhi: Government of Malawi: Ministry of Health and Population; 2018.
-
- Mziray E, Gorgens M, McCauley P. Analysis of human resources for health in Malawi. Washington, DC: World Bank; 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
