

Design and baseline characteristics of the ILD-PRO registry in patients with progressive pulmonary fibrosis
- PMID: 39334205
- PMCID: PMC11438290
- DOI: 10.1186/s12890-024-03247-8
Design and baseline characteristics of the ILD-PRO registry in patients with progressive pulmonary fibrosis
Abstract
Background: To assess the characteristics of patients enrolled in the ILD-PRO Registry.
Methods: The ILD-PRO Registry is a multicentre US registry of patients with progressive pulmonary fibrosis. This registry is enrolling patients with an interstitial lung disease (ILD) other than idiopathic pulmonary fibrosis who have reticular abnormality and traction bronchiectasis on HRCT, and who meet criteria for ILD progression within the prior 24 months. Patient characteristics were analysed based on the number of patients with available data.
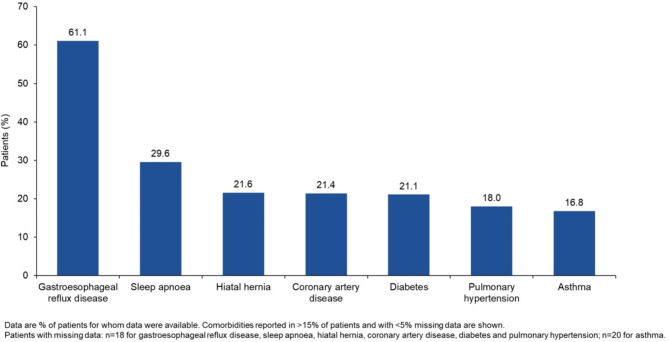
Results: Of the first 491 patients enrolled, the majority were white (75.4%) and female (60.6%); 47.4% had a history of smoking. Reported ILDs were autoimmune disease-associated ILDs (47.2%), hypersensitivity pneumonitis (17.5%), idiopathic non-specific interstitial pneumonia (9.1%), interstitial pneumonia with autoimmune features (8.9%), unclassifiable ILD (7.6%), other ILDs (9.7%). At enrolment, median (Q1, Q3) FVC % predicted was 62.2 (49.4, 72.4) and DLco % predicted was 39.2 (30.2, 49.2). Median (Q1, Q3) total score on the St. George's Respiratory Questionnaire was 50.8 (35.9, 64.7). The most common comorbidities were gastroesophageal reflux disease (61.1%) and sleep apnoea (29.6%). Overall, 64.5% of patients were receiving immunosuppressive or cytotoxic therapy, 61.1% proton-pump inhibitors, 53.2% oral steroids, 19.8% nintedanib and 3.6% pirfenidone.
Conclusions: Patients enrolled into the ILD-PRO Registry have a variety of ILD diagnoses, marked impairment in lung function and health-related quality of life, and high medication use. Longitudinal data from this registry will further our knowledge of the course of progressive pulmonary fibrosis.
Trial registration: ClinicalTrials.gov, NCT01915511; registered August 5, 2013.
Keywords: Clinical trial; Disease progression; Interstitial lung disease; Pulmonary fibrosis.
© 2024. The Author(s).
Conflict of interest statement
L Jason Lobo, Murali Ramaswamy and Srihari Veeraraghavan are principal investigators in the IPF-PRO/ILD-PRO Registry. Srihari Veeraraghavan also reports research funding paid to Emory Healthcare from Bellerophon Therapeutics, Boehringer Ingelheim, FibroGen, Galactic, Galapagos, Nitto Denko Avecia, Pliant, United Therapeutics; consultancy fees for serving on advisory boards from Boehringer Ingelheim and United Therapeutics; and serves on the Georgia leadership board for the American Lung Association. Yi Liu, Peide Li, Yanni Fan and Amy L Olson are employees of Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI). Aparna C Swaminathan, Megan L Neely and Scott M Palmer are faculty members of the Duke Clinical Research Institute (DCRI), which receives funding support from BIPI to coordinate the IPF-PRO/ILD-PRO Registry. Aparna C Swaminathan also reports consultancy fees from United Therapeutics. Scott M Palmer also reports research funding paid to DCRI from Bristol Myers Squibb and Genentech and has participated on advisory boards for Altavant and Bristol Myers Squibb.
Figures




References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
