

The INTOXICATE study: methodology and preliminary results of a prospective observational study
- PMID: 39334221
- PMCID: PMC11430428
- DOI: 10.1186/s13054-024-05096-7
The INTOXICATE study: methodology and preliminary results of a prospective observational study
Abstract
Background: There is currently no practice-based, multicenter database of poisoned patients admitted to intensive care units (ICUs). The INTOXICATE study, endorsed by the ESICM and EAPCCT, aimed to determine the rate of eventful admissions among acutely intoxicated adult ICU patients.
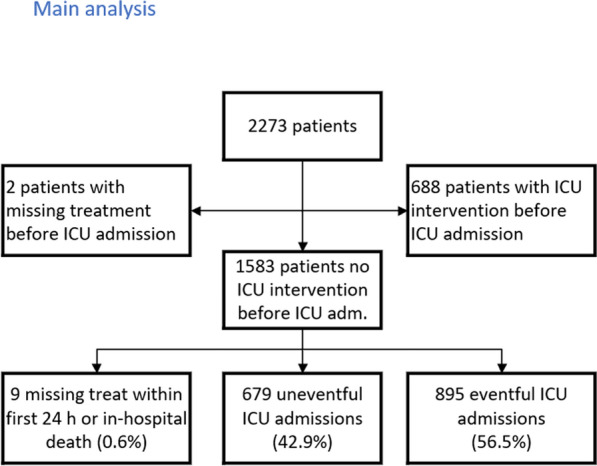
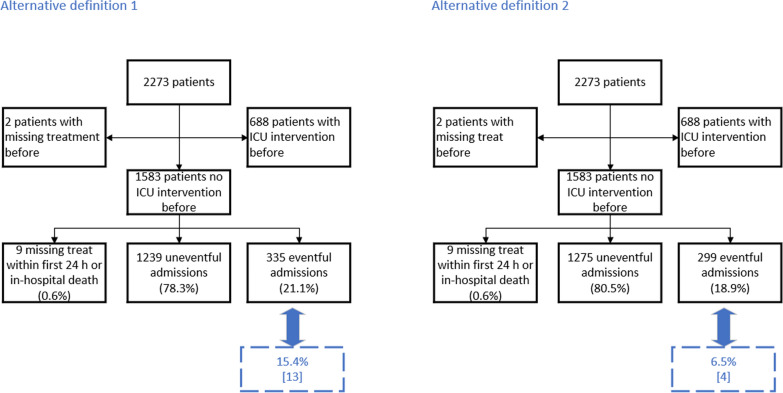
Methods: Ethical approval was obtained for this multicenter, prospective observational study, and data-sharing agreements were signed with each participating center. An electronic case report form was used to collect data on patient demographics, exposure, clinical characteristics, investigations, treatment, and in-hospital mortality data. The primary outcome, 'eventful admission', was a composite outcome defined as the rate of patients who received any of the following treatments in the first 24 h after the ICU admission: oxygen supplementation with a FiO2 > 40%, mechanical ventilation, vasopressors, renal replacement therapy (RRT), cardiopulmonary resuscitation, antidotes, active cooling, fluid resuscitation (> 1.5 L of intravenous fluid of any kind), sedation, or who died in the hospital.
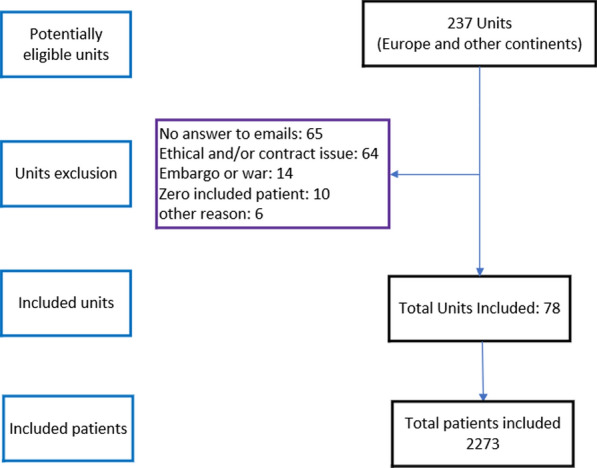
Results: Seventy-eight ICUs, mainly from Europe, but also from Australia and the Eastern Mediterranean, participated. A total of 2,273 patients were enrolled between November 2020 and June 2023. The median age of the patients was 41 years, 72% were exposed to intoxicating drugs. The observed rate of patients with an eventful ICU admission was 68% (n = 1546/2273 patients). The hospital mortality was 4.5% (n = 103/2273).
Conclusions: The vast majority of patients survive, and approximately one third of patients do not receive any ICU-specific interventions after admission in an intensive care unit for acute intoxication. High-quality detailed clinical data have been collected from a large cohort of acutely intoxicated ICU patients, providing information on the pattern of severe acute poisoning requiring intensive care admission and the outcomes of these patients.
Trial registration: OSF registration ID: osf.io/7e5uy.
Keywords: Critical care outcomes; Database management systems; Intensive care units; Poisoning; Toxicology.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
