

Functional heterogeneity of cancer-associated fibroblasts with distinct neoadjuvant immunotherapy plus chemotherapy response in esophageal squamous cell carcinoma
- PMID: 39334513
- PMCID: PMC11437904
- DOI: 10.1186/s40364-024-00656-z
Functional heterogeneity of cancer-associated fibroblasts with distinct neoadjuvant immunotherapy plus chemotherapy response in esophageal squamous cell carcinoma
Abstract
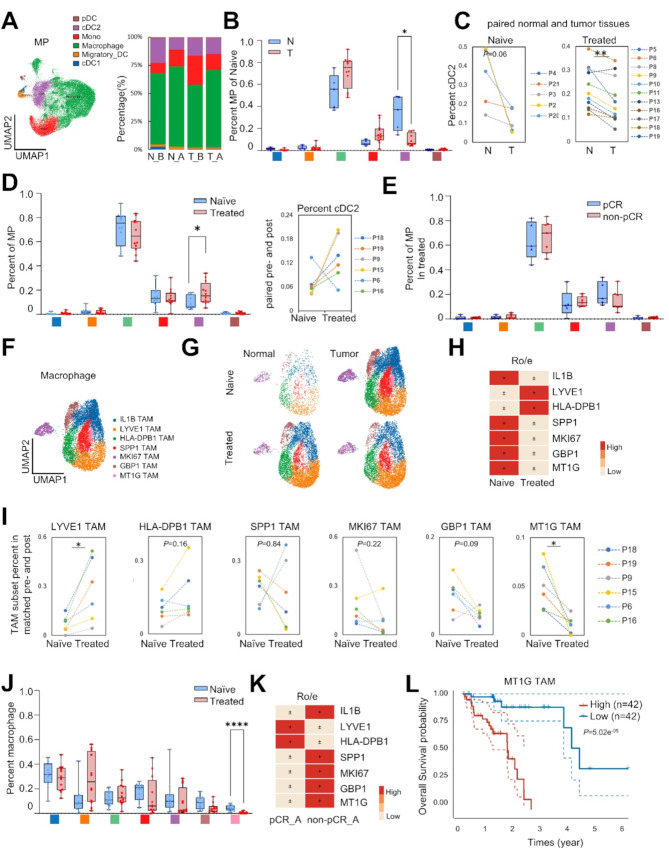
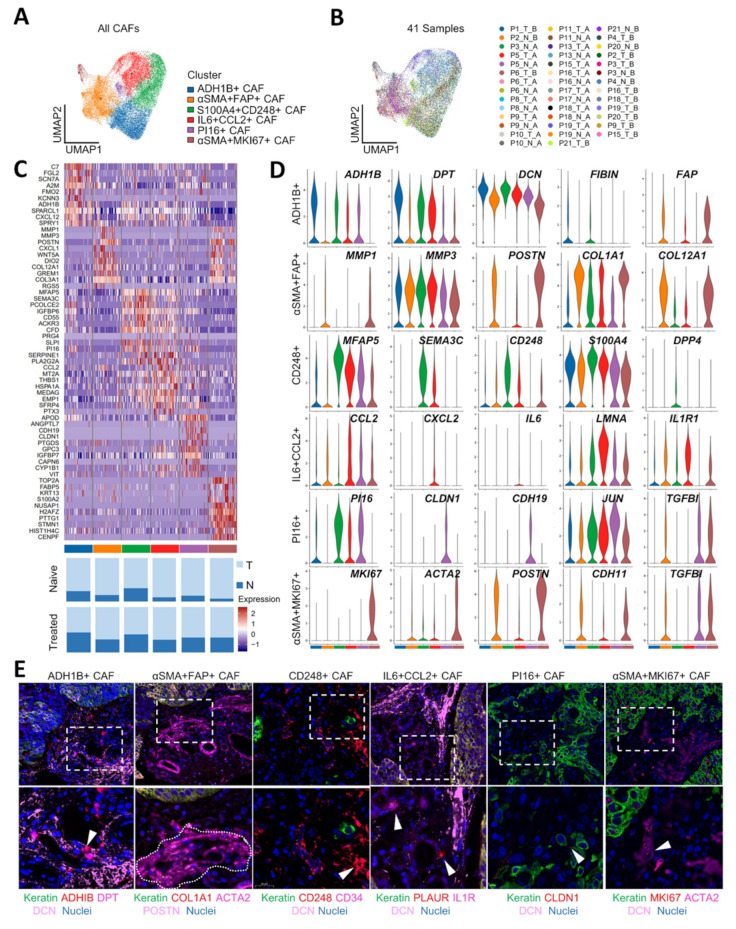
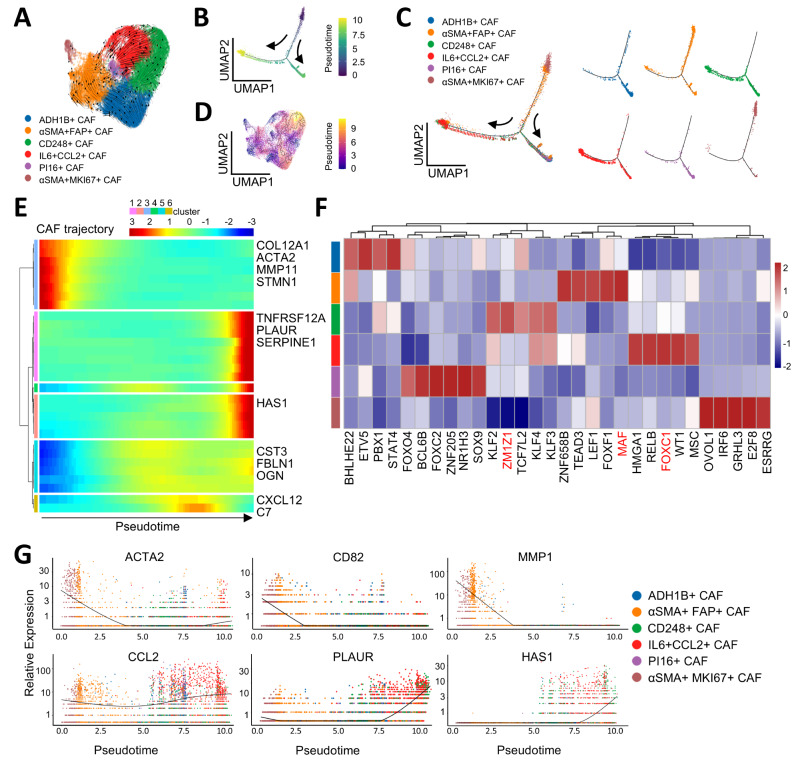
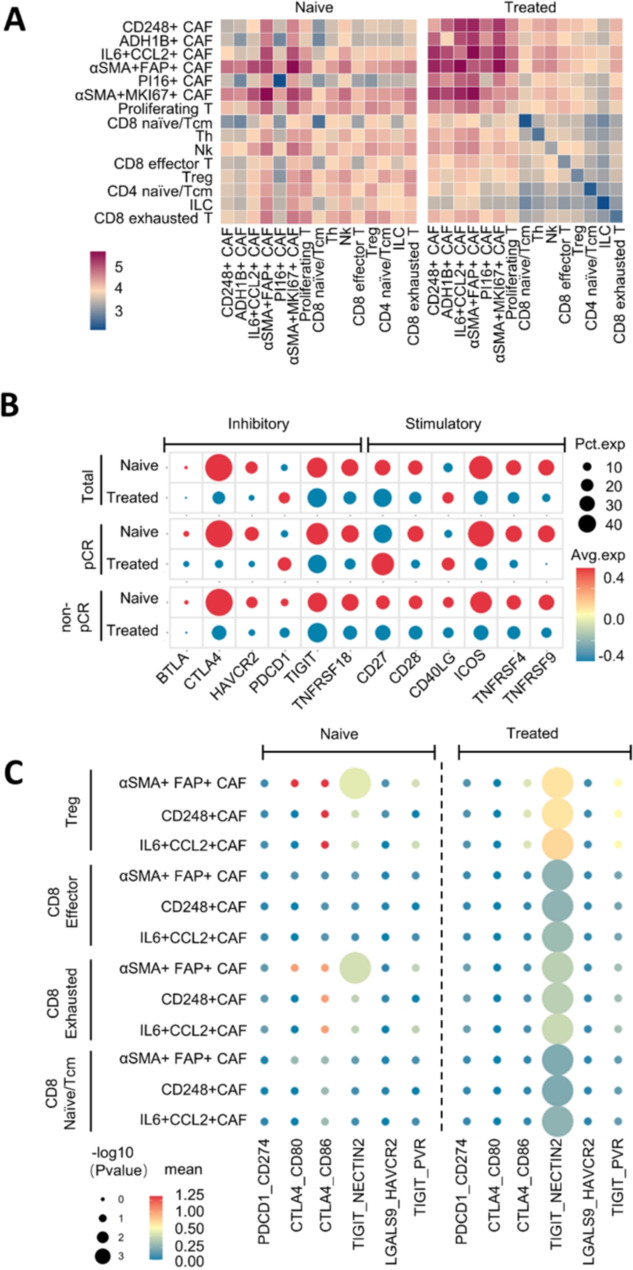
Novel neoadjuvant immunotherapy combined with chemotherapy (neoICT) has improved outcomes for patients with esophageal squamous-cell carcinoma (ESCC), but challenges persist in low response rates and therapy resistance. Little is known about the intra-tumoral heterogeneity in the ESCC tumor microenvironment (TME) that underlies differential responses to neoadjuvant therapy. We applied single-cell RNA sequencing (scRNA-seq) profiling and multiplexed immunofluorescence staining to thoroughly decipher the TME in ESCC specimens from a neoadjuvant anti-PD1 combination therapy clinical trial. The cancer-associated fibroblasts (CAFs) population showed the significant alteration in abundance following neoadjuvant therapy. Specifically, IL6 + CCL2 + immunomodulatory CAFs and a novel CD248 + mechanoresponsive CAFs subset exhibited increasing infiltration. Mechanistically, CD248 + mechanoresponsive CAFs approached and lined the tumor nest to physically block the infiltration of CD8 + T cells and drug delivery, while IL6 + CCL2 + immunomodulatory CAFs induced therapeutic resistance with distinct IL-6 expression. Among patients treated with neoICT, we observed prominent CAF-T cell interactions. In particular, the NECTIN2-TIGIT ligand-receptor pair was enriched in treated samples, and TIGIT was identified as the major inhibitory checkpoint of T cells. Our findings demonstrate distinct alterations in TME constituent responses to neoadjuvant immunotherapy and identify functional phenotypes of CAFs associated with unfavorable therapeutic responses in patients. This provides potential targets to enhance responses to neoadjuvant therapy in ESCC.
Keywords: Cancer-associated fibroblasts; Esophageal squamous-cell carcinoma; Neoadjuvant immunochemotherapy; Tumor microenvironment; scRNA-seq.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. Cancer J Clin. 2021;71(3):209–49. 10.3322/caac.21660. - PubMed
-
- Pennathur A, Gibson MK, Jobe BA, Luketich JD. Oesophageal carcinoma. Lancet (London England). 2013;381(9864):400–12. 10.1016/s0140-6736(12)60643-6. - PubMed
-
- Arnold M, Ferlay J, van Berge Henegouwen MI, Soerjomataram I. Global burden of oesophageal and gastric cancer by histology and subsite in 2018. Gut. 2020;69(9):1564–71. 10.1136/gutjnl-2020-321600. - PubMed
-
- Doki Y, Ajani JA, Kato K, Xu J, Wyrwicz L, Motoyama S, et al. Nivolumab Combination Therapy in Advanced Esophageal squamous-cell carcinoma. N Engl J Med. 2022;386(5):449–62. 10.1056/NEJMoa2111380. - PubMed
-
- Kato K, Cho BC, Takahashi M, Okada M, Lin CY, Chin K, et al. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20(11):1506–17. 10.1016/s1470-2045(19)30626-6. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
