

The Constellation of Risk Factors and Paraneoplastic Syndromes in Cholangiocarcinoma: Integrating the Endocrine Panel Amid Tumour-Related Biology (A Narrative Review)
- PMID: 39336089
- PMCID: PMC11429066
- DOI: 10.3390/biology13090662
The Constellation of Risk Factors and Paraneoplastic Syndromes in Cholangiocarcinoma: Integrating the Endocrine Panel Amid Tumour-Related Biology (A Narrative Review)
Abstract
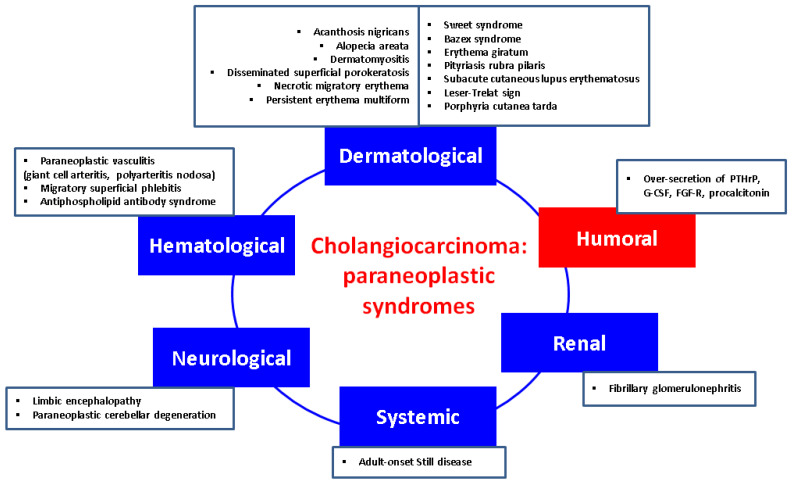
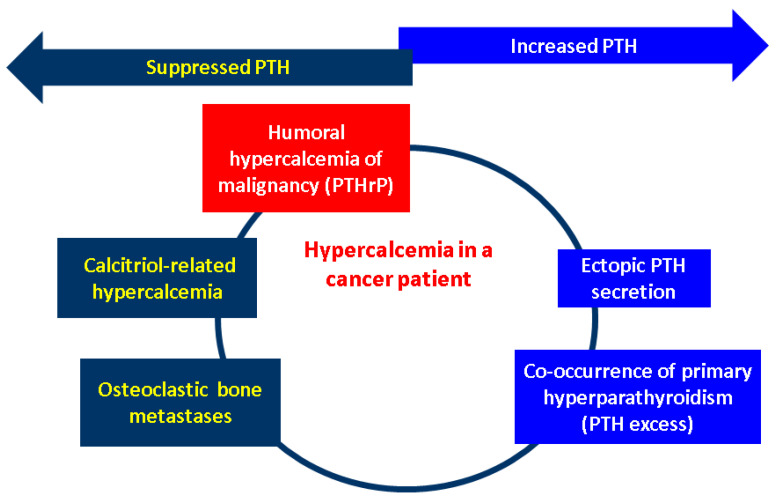
Cholangiocarcinomas (CCAs), a heterogeneous group of challenging malignant tumours which originate from the biliary epithelium, are associated with an alarming increasing incidence during recent decades that varies between different regions of the globe. Thus, awareness represents the key operating factor. Our purpose was to overview the field of CCAs following a double perspective: the constellation of the risk factors, and the presence of the paraneoplastic syndromes, emphasizing the endocrine features amid the entire multidisciplinary panel. This is a narrative review. A PubMed-based search of English-language original articles offered the basis of this comprehensive approach. Multiple risk factors underlying different levels of statistical evidence have been listed such as chronic biliary diseases and liver conditions, inflammatory bowel disease, parasitic infections (e.g., Opisthorchis viverrini, Clonorchis sinensis), lifestyle influence (e.g., alcohol, smoking), environmental exposure (e.g., thorotrast, asbestos), and certain genetic and epigenetic interplays. With regard to the endocrine panel, a heterogeneous spectrum should be taken into consideration: non-alcoholic fatty liver disease, obesity, type 2 diabetes mellitus, and potential connections with vitamin D status, glucagon-like peptide 1 receptor, or the galanin system, respectively, with exposure to sex hormone therapy. Amid the numerous dermatologic, hematologic, renal, and neurologic paraneoplastic manifestations in CCAs, the endocrine panel is less described. Humoral hypercalcaemia of malignancy stands as the most frequent humoral paraneoplastic syndrome in CCAs, despite being exceptional when compared to other paraneoplastic (non-endocrine) manifestations and to its reported frequency in other (non-CCAs) cancers (it accompanies 20-30% of all cancers). It represents a poor prognosis marker in CCA; it may be episodic once the tumour relapses. In addition to the therapy that targets the originating malignancy, hypercalcaemia requires the administration of bisphosphonates (e.g., intravenous zoledronic acid) or denosumab. Early detection firstly helps the general wellbeing of a patient due to a prompt medical control of high serum calcium and it also provides a fine biomarker of disease status in selected cases that harbour the capacity of PTHrP secretion. The exact molecular biology and genetic configuration of CCAs that display such endocrine traits is still an open matter, but humoral hypercalcaemia adds to the overall disease burden.
Keywords: PTHrP; calcium; cholangiocarcinoma; endocrine; paraneoplastic syndrome; risk factor; tumour biology.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Izquierdo-Sanchez L., Lamarca A., La Casta A., Buettner S., Utpatel K., Klümpen H.J., Adeva J., Vogel A., Lleo A., Fabris L., et al. Cholangiocarcinoma landscape in Europe: Diagnostic, prognostic and therapeutic insights from the ENSCCA Registry. J. Hepatol. 2022;76:1109–1121. doi: 10.1016/j.jhep.2021.12.010. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
