

Silent Threats of the Heart: A Case Series and Narrative Review on Suicide Left Ventricle Post-Aortic Valve Replacement in Patients with Dynamic LVOT Obstruction and Aortic Stenosis
- PMID: 39337045
- PMCID: PMC11432347
- DOI: 10.3390/jcm13185555
Silent Threats of the Heart: A Case Series and Narrative Review on Suicide Left Ventricle Post-Aortic Valve Replacement in Patients with Dynamic LVOT Obstruction and Aortic Stenosis
Abstract
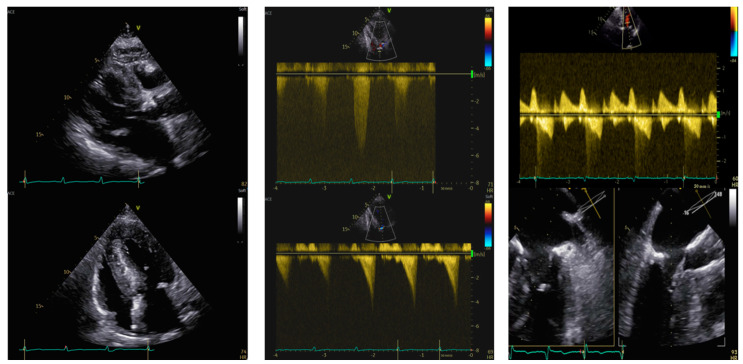
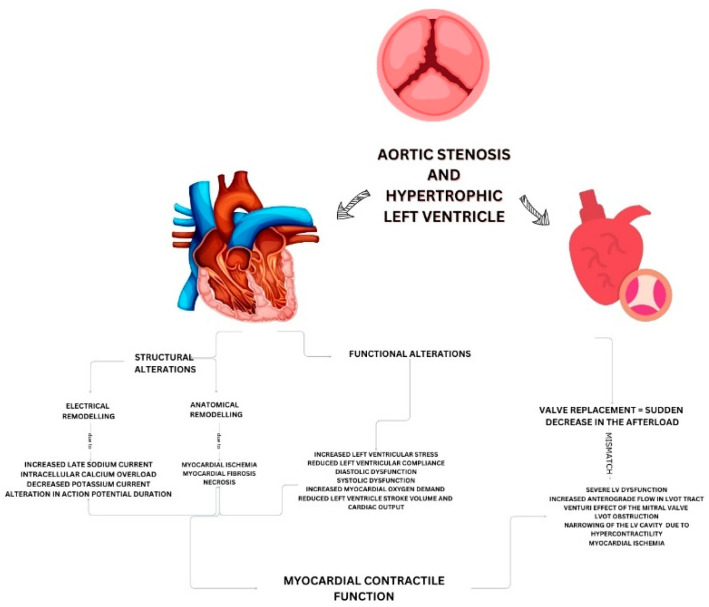
Aortic stenosis (AS) is the most prevalent valvular heart disease in Europe and North America, with transcatheter aortic valve implantation (TAVI) revolutionizing its management. Hypertrophic left ventricle (HLV) frequently coexists with AS, complicating treatment due to the associated risk of left ventricular outflow tract (LVOT) obstruction, heart failure, and sudden death. A rare but severe post-aortic valve replacement (AVR) complication, termed "suicide left ventricle" (SLV), has emerged, necessitating further study. This report synthesizes current literature on SLV, its pathophysiology, and management strategies, alongside four patient case studies. The patients aged 79-87 years, underwent AVR for symptomatic AS with HLV. Post-AVR, all experienced severe complications, including dynamicLVOT gradients, systolic anterior motion (SAM) of the mitral valve, and severe hypotension, leading to death in two cases. One patient survived following surgical aortic valve replacement (SAVR) with surgical myectomy. One patient survived after TAVI. These cases highlight the critical importance of multidisciplinary Heart Team evaluations and personalized treatment plans in managing SLV. Despite advancements in AVR, SLV remains a complex, life-threatening condition, requiring an exhaustive and multifaceted approach for optimal patient outcomes. This report offers valuable insights into SLV occurrence and management from a clinical perspective.
Keywords: aortic stenosis; hypertrophic left ventricle; multidisciplinary management; suicide left ventricle.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Vora A.N., Gada H., Manandhar P., Kosinski A., Kirtane A., Nazif T., Reardon M., Kodali S., Cohen D.J., Thourani V., et al. National Variability in Pacemaker Implantation Rate Following TAVR: Insights From the STS/ACC TVT Registry. JACC Cardiovasc. Interv. 2024;17:391–401. doi: 10.1016/j.jcin.2023.12.005. - DOI - PubMed
-
- Huded C.P., Arnold S.V., Cohen D.J., Manandhar P., Vemulapalli S., Saxon J.T., Chhatriwalla A.K., Kosinski A., Spertus J.A. Outcomes of Transcatheter Aortic Valve Replacement in Asymptomatic or Minimally Symptomatic Aortic Stenosis. JACC Cardiovasc. Interv. 2023;16:2631–2641. doi: 10.1016/j.jcin.2023.07.007. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
