

Lactic Acid Bacteria-Gut-Microbiota-Mediated Intervention towards Inflammatory Bowel Disease
- PMID: 39338538
- PMCID: PMC11433943
- DOI: 10.3390/microorganisms12091864
Lactic Acid Bacteria-Gut-Microbiota-Mediated Intervention towards Inflammatory Bowel Disease
Abstract
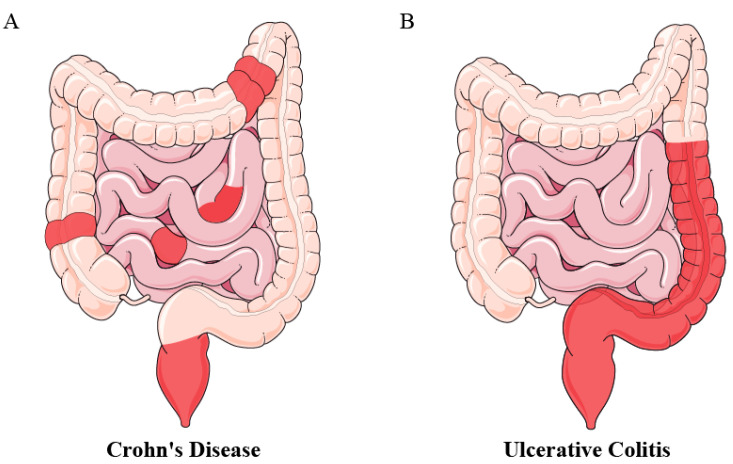
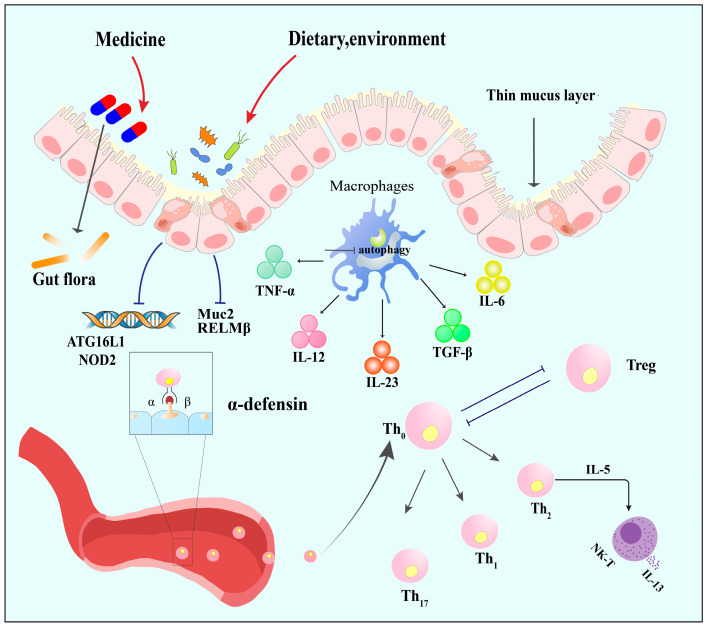
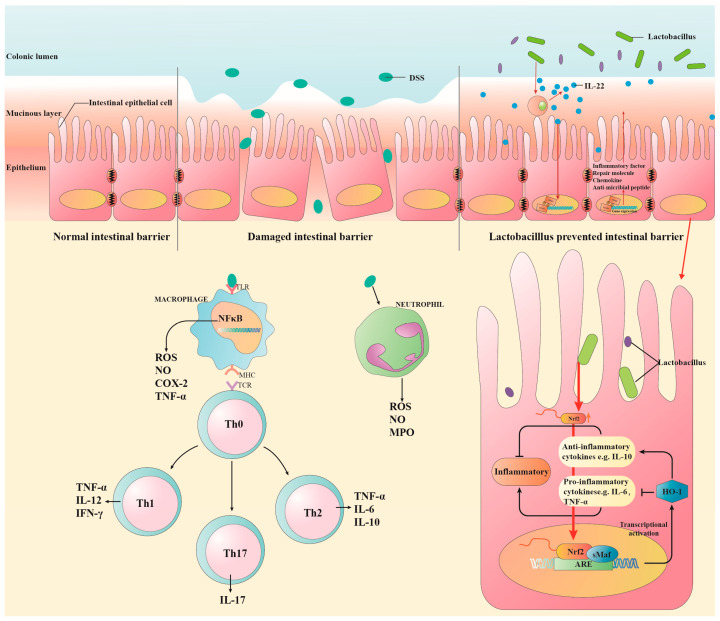
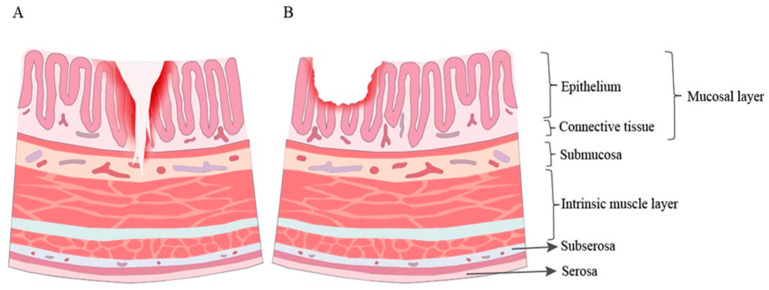
Inflammatory bowel disease (IBD), encompassing ulcerative colitis (UC) and Crohn's disease (CD), arises from intricate interactions involving genetics, environment, and pharmaceuticals with an ambiguous pathogenic mechanism. Recently, there has been an increasing utilization of lactic acid bacteria (LAB) in managing IBD, attributed to their ability to enhance intestinal barrier function, mitigate inflammatory responses, and modulate gut microbiota. This review initiates by elucidating the pathogenesis of IBD and its determinants, followed by an exploration of the mechanisms underlying LAB therapy in UC and CD. Special attention is directed towards their influence on intestinal barrier function and homeostasis regulated by gut microbiota. Furthermore, the review investigates the complex interplay among pivotal gut microbiota, metabolites, and pathways associated with inflammation. Moreover, it underscores the limitations of LAB in treating IBD, particularly in light of their varying roles in UC and CD. This comprehensive analysis endeavors to offer insights for the optimized application of LAB in IBD therapy.
Keywords: Crohn’s disease; inflammatory bowel disease; lactic acid bacteria; ulcerative colitis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Saez-Lara M.J., Gomez-Llorente C., Plaza-Diaz J., Gil A. The Role of Probiotic Lactic Acid Bacteria and Bifidobacteria in the Prevention and Treatment of Inflammatory Bowel Disease and Other Related Diseases: A Systematic Review of Randomized Human Clinical Trials. BioMed Res. Int. 2015;2015:505878. doi: 10.1155/2015/505878. - DOI - PMC - PubMed
-
- Raffals L.E., Saha S., Bewtra M., Norris C., Dobes A., Heller C., O’Charoen S., Fehlmann T., Sweeney S., Weaver A., et al. The Development and Initial Findings of a Study of a Prospective Adult Research Cohort with Inflammatory Bowel Disease (SPARC IBD) Inflamm. Bowel Dis. 2021;28:192–199. doi: 10.1093/ibd/izab071. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
