

Cytomegalovirus Retinitis: Clinical Manifestations, Diagnosis and Treatment
- PMID: 39339903
- PMCID: PMC11437412
- DOI: 10.3390/v16091427
Cytomegalovirus Retinitis: Clinical Manifestations, Diagnosis and Treatment
Abstract
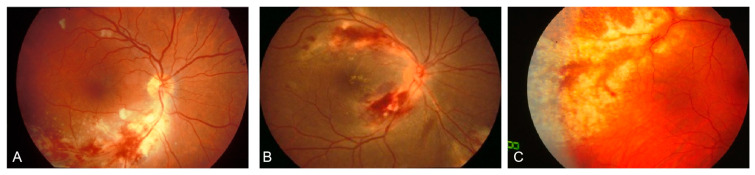
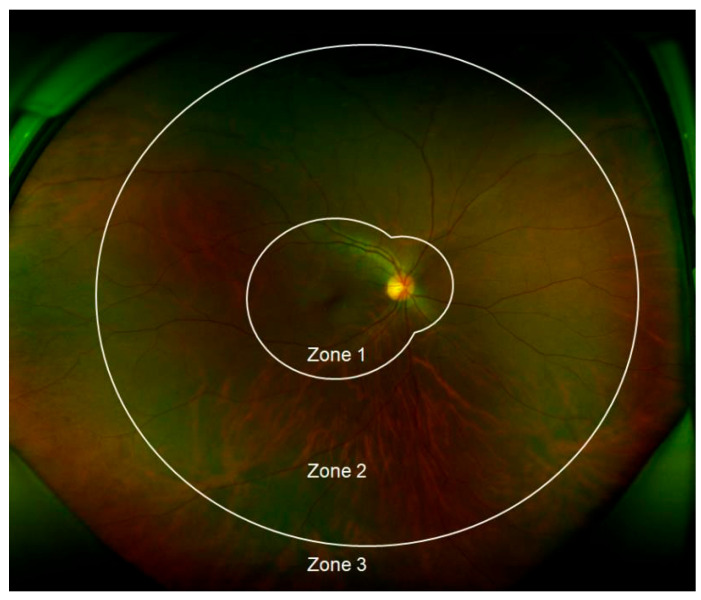
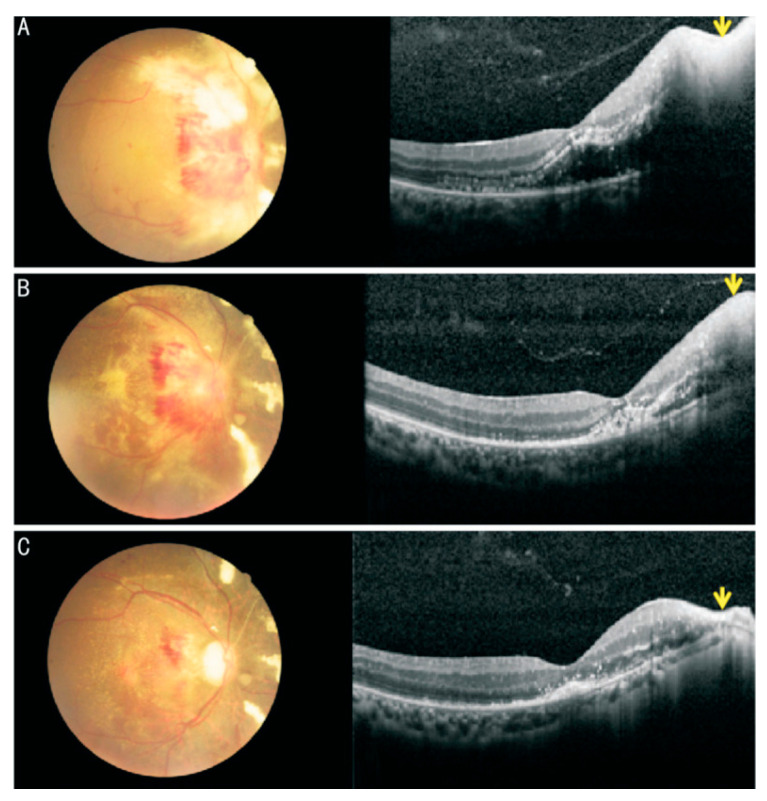
Cytomegalovirus (CMV) retinitis is the most common eye disease associated with CMV infection in immunocompromised individuals. The CMVR may initially be asymptomatic; however, relatively mild vitreous inflammation at the onset may be an important differential point from other diseases in HIV patients. Fundus photography, CD4 T-cell count, and telemedicine could be used to screen and monitor the high-risk population, particularly in resource-limited regions. Retinitis generally starts in the peripheral retina and advances toward the posterior pole, which could develop to the characteristic "pizza pie" appearance marked by central retinal necrosis and intraretinal hemorrhage. CMVR causes vision loss if left untreated, and early antiviral therapy significantly reduces the risk of vision loss. Alongside traditional antiviral treatments, immunotherapies including CMV-specific adoptive T-cell therapy and CMV immunoglobulin (CMVIG) are emerging as promising treatment options due to their favorable tolerability and reduced mortality. This review comprehensively examines CMV retinitis, encompassing the clinical features, differential diagnosis, laboratory tests, and updated treatment strategies to inform clinical management.
Keywords: antiviral treatment; cytomegalovirus; differential diagnosis; immunodeficiency; retinitis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
