

Immunity to Varicella Zoster Virus in Healthcare Workers: A Systematic Review and Meta-Analysis (2024)
- PMID: 39340051
- PMCID: PMC11436139
- DOI: 10.3390/vaccines12091021
Immunity to Varicella Zoster Virus in Healthcare Workers: A Systematic Review and Meta-Analysis (2024)
Abstract
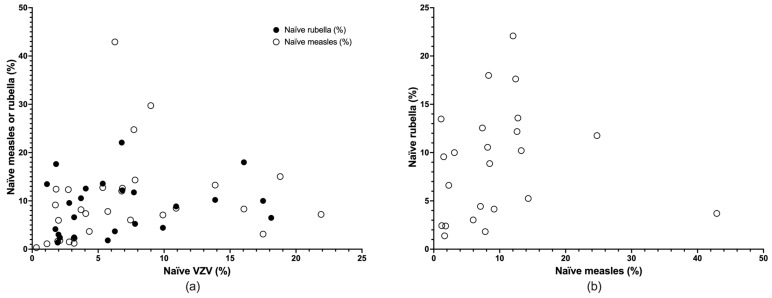
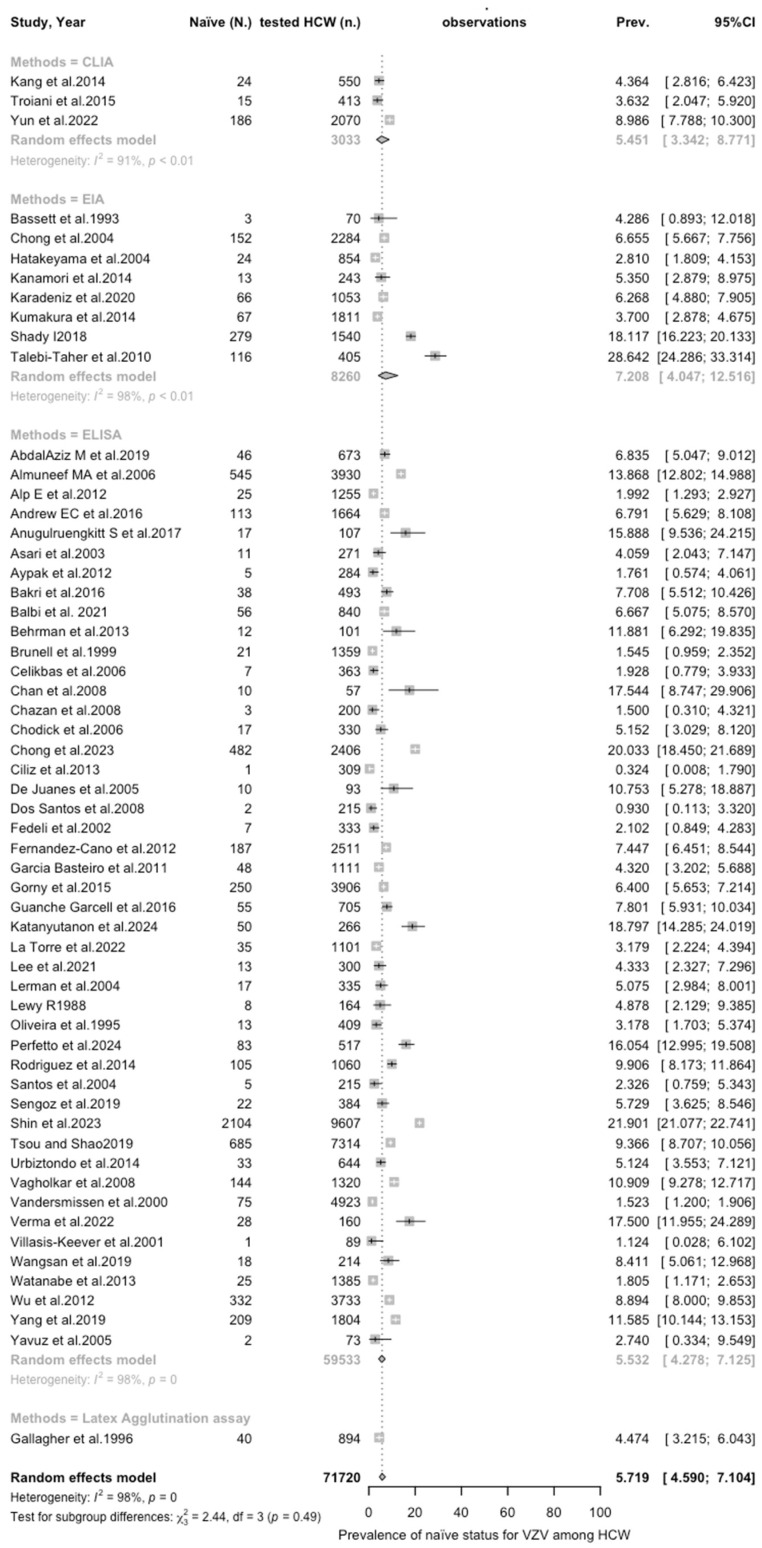
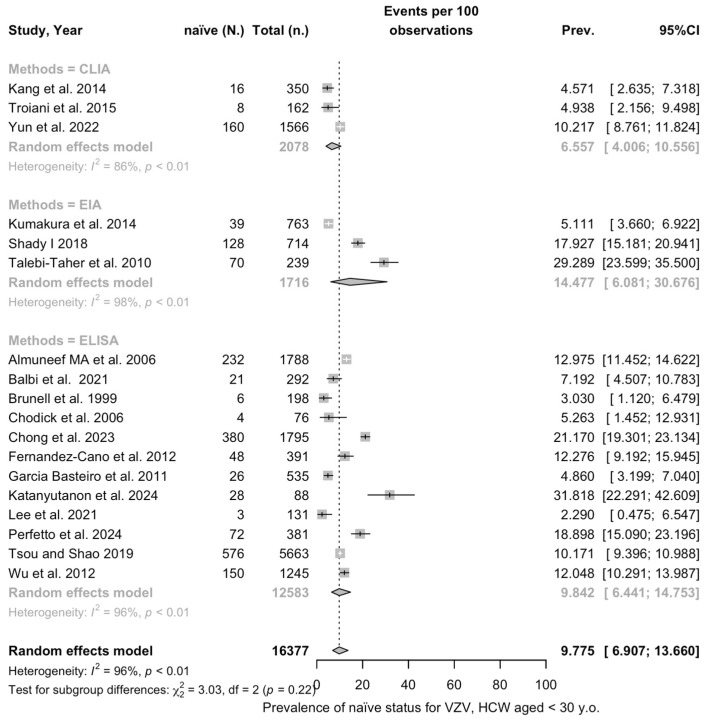
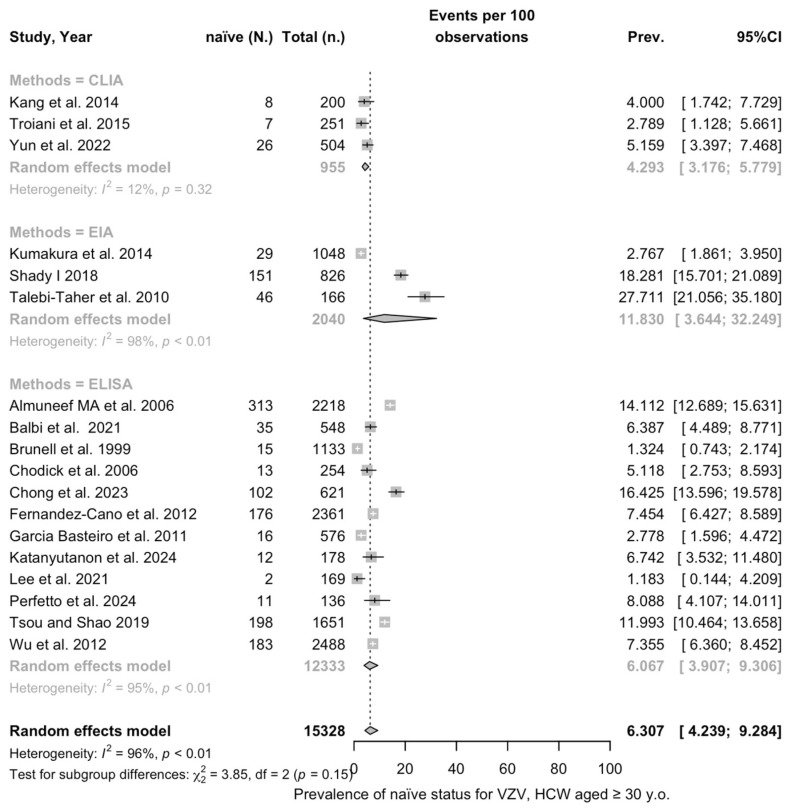
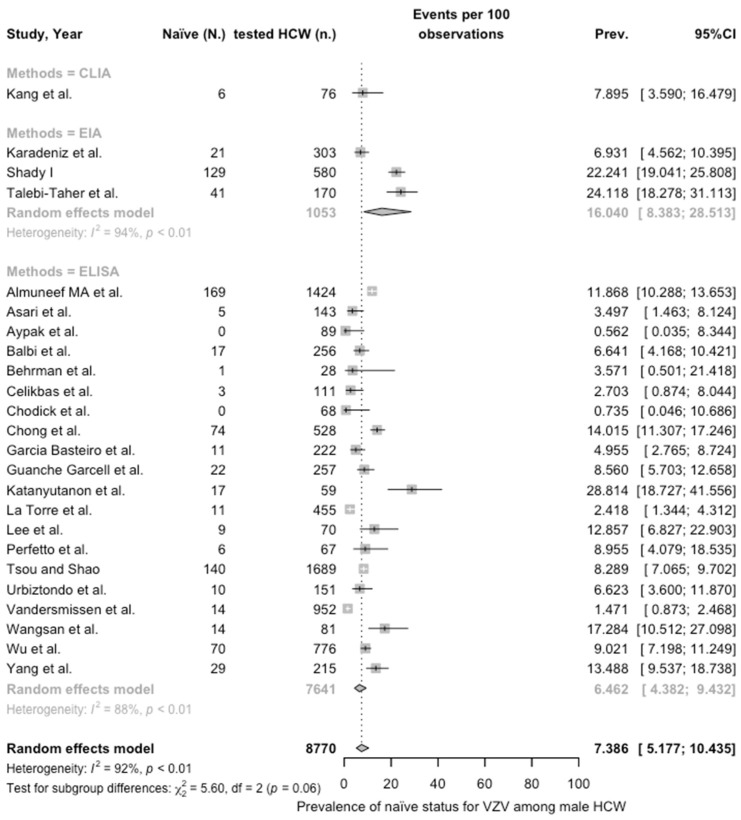
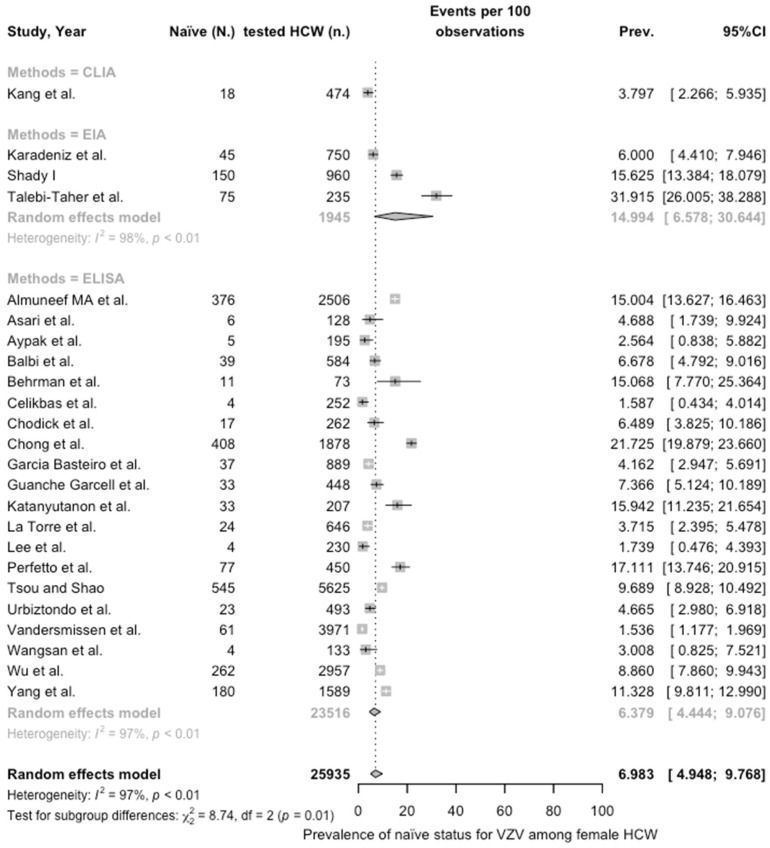
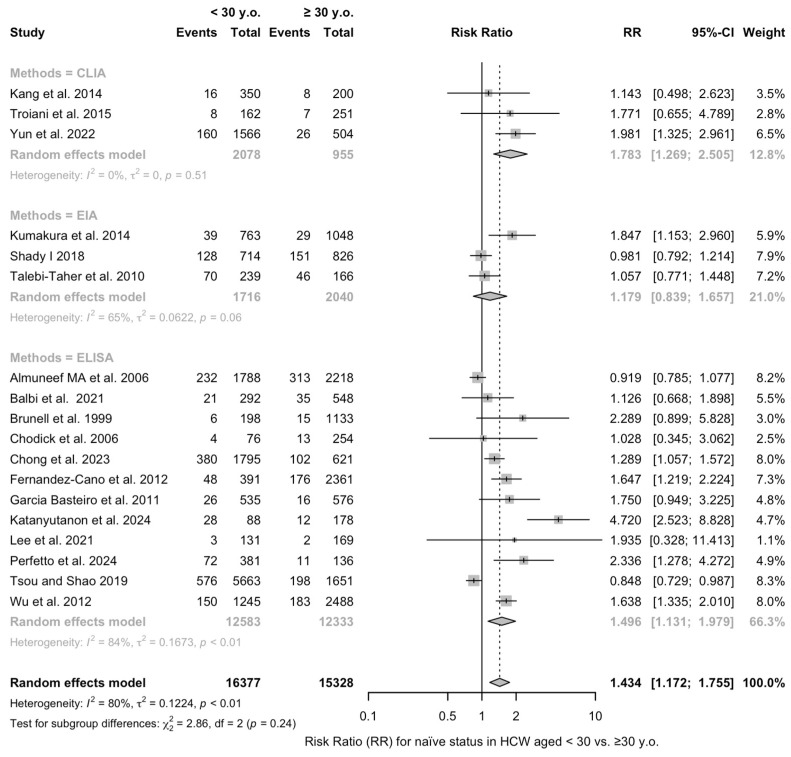
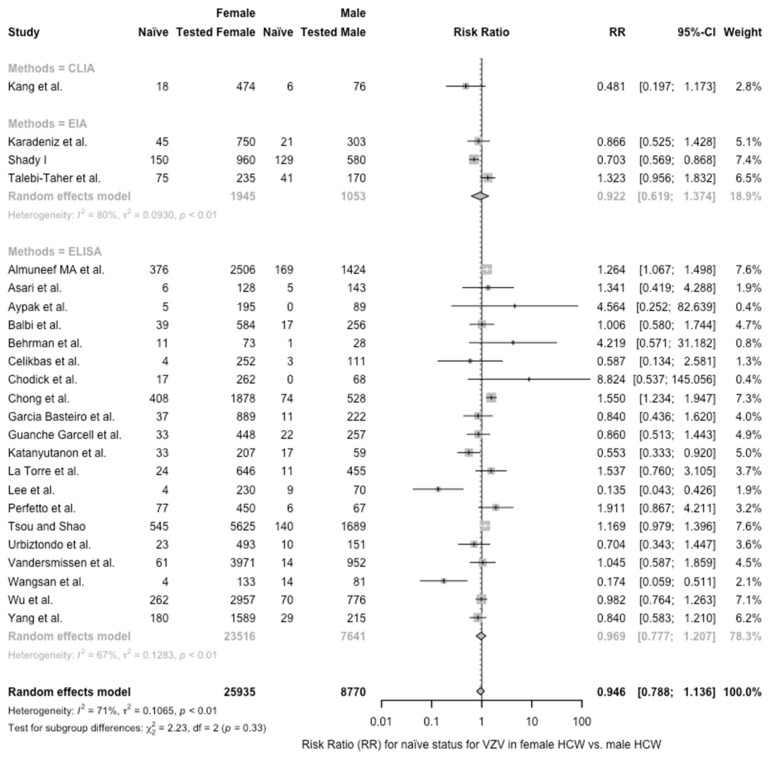
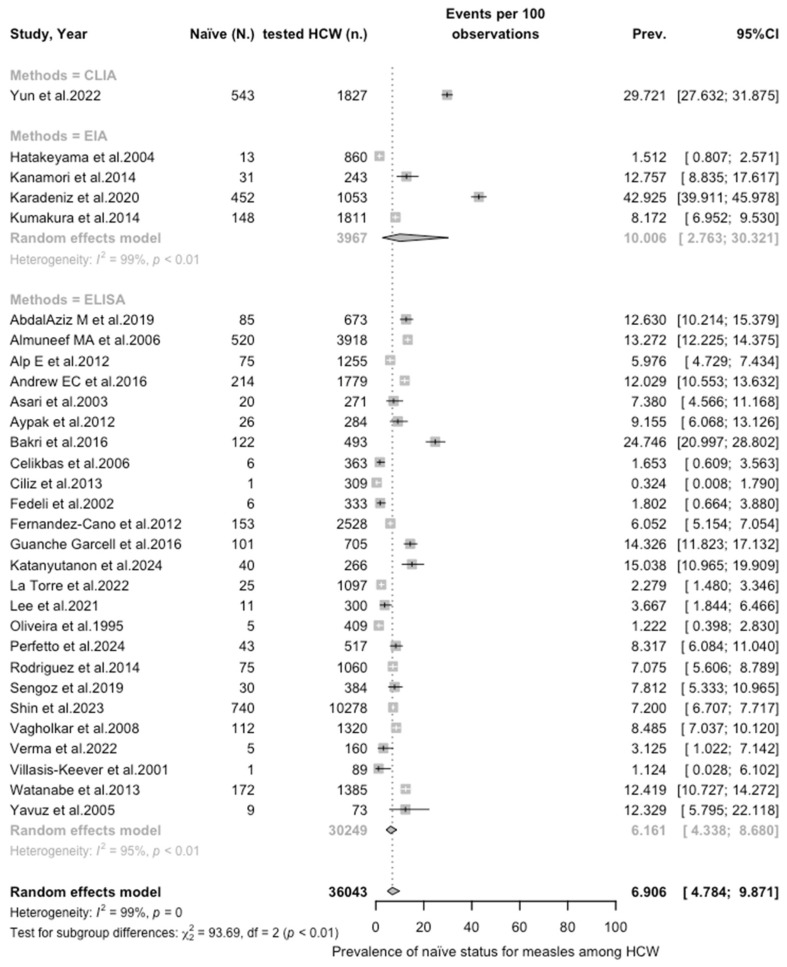
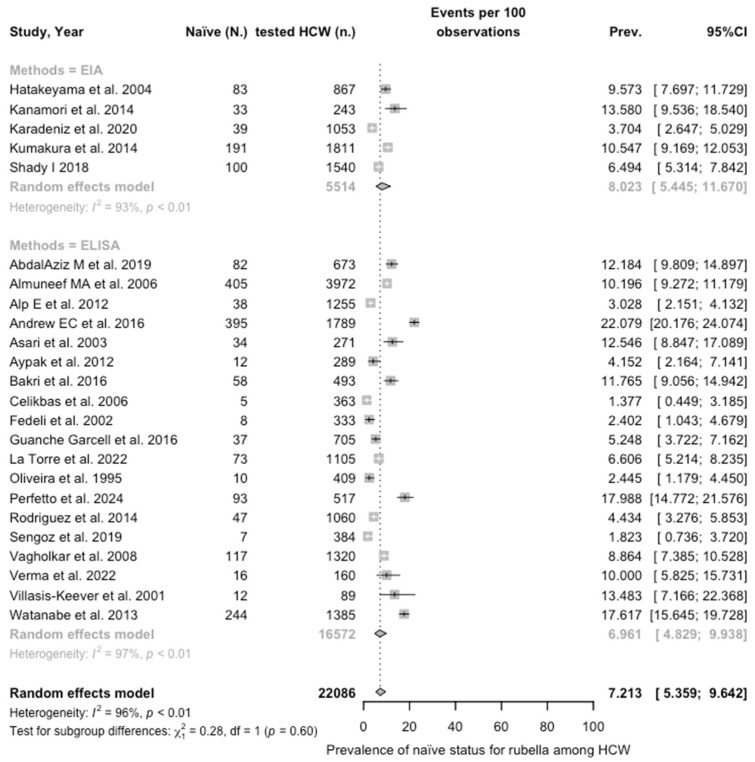
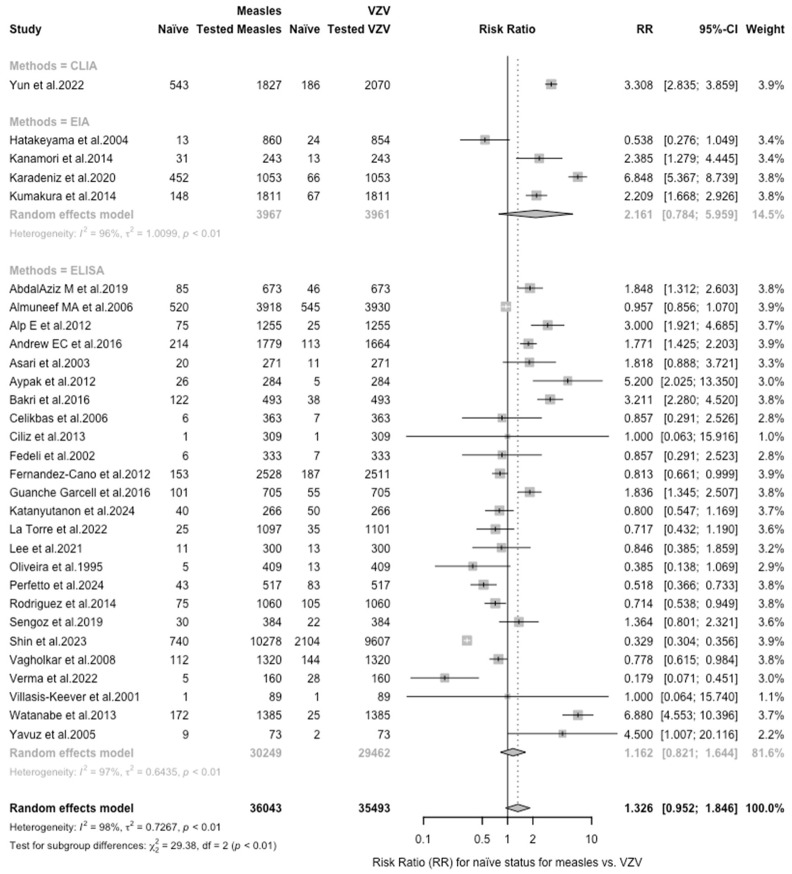
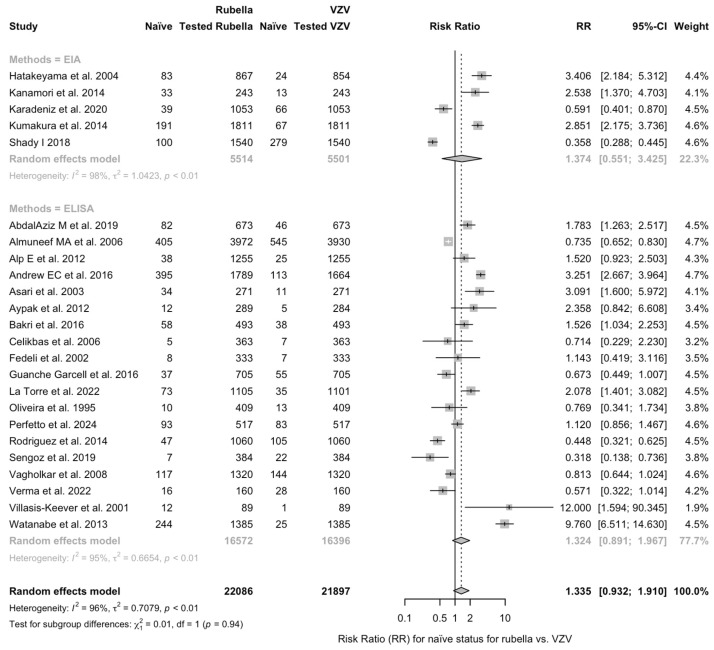
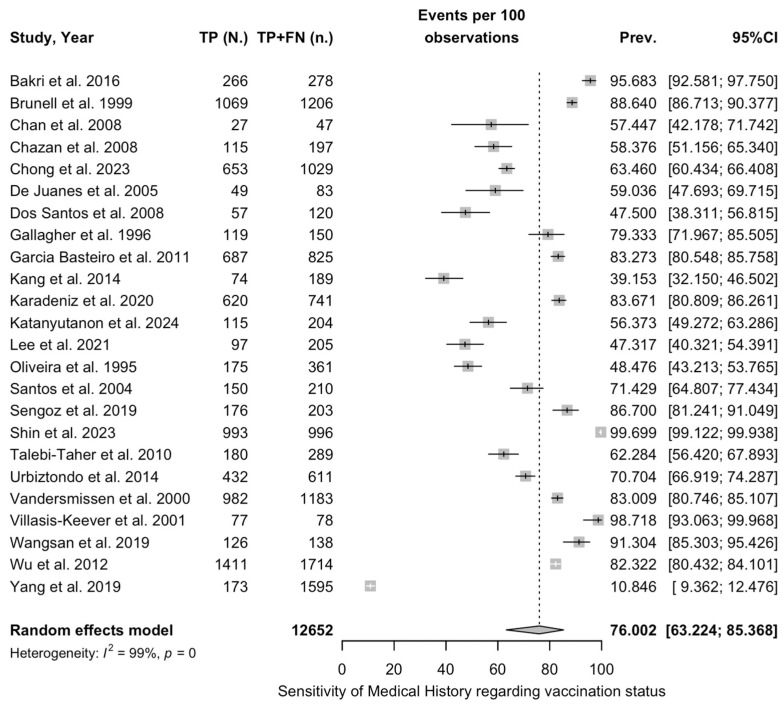
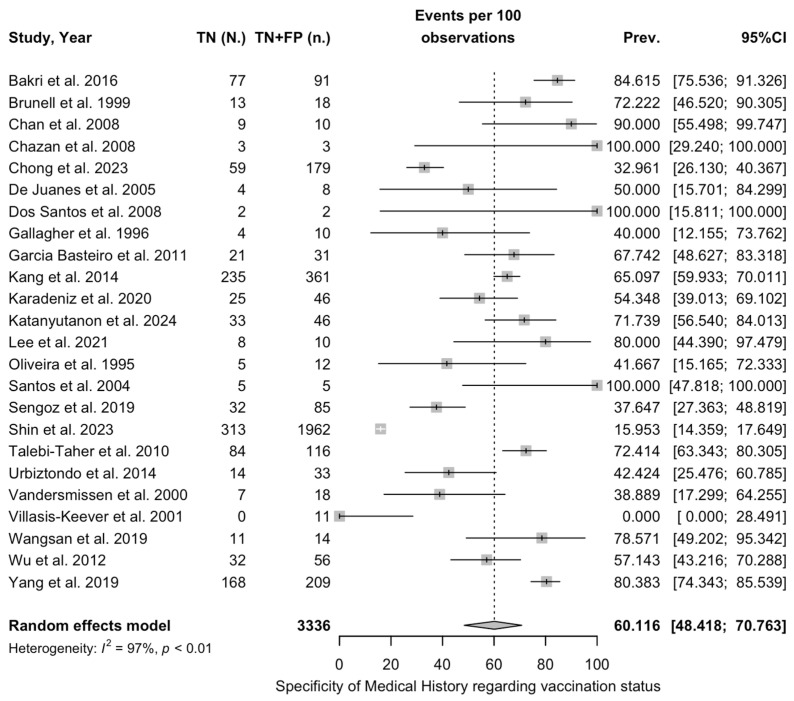
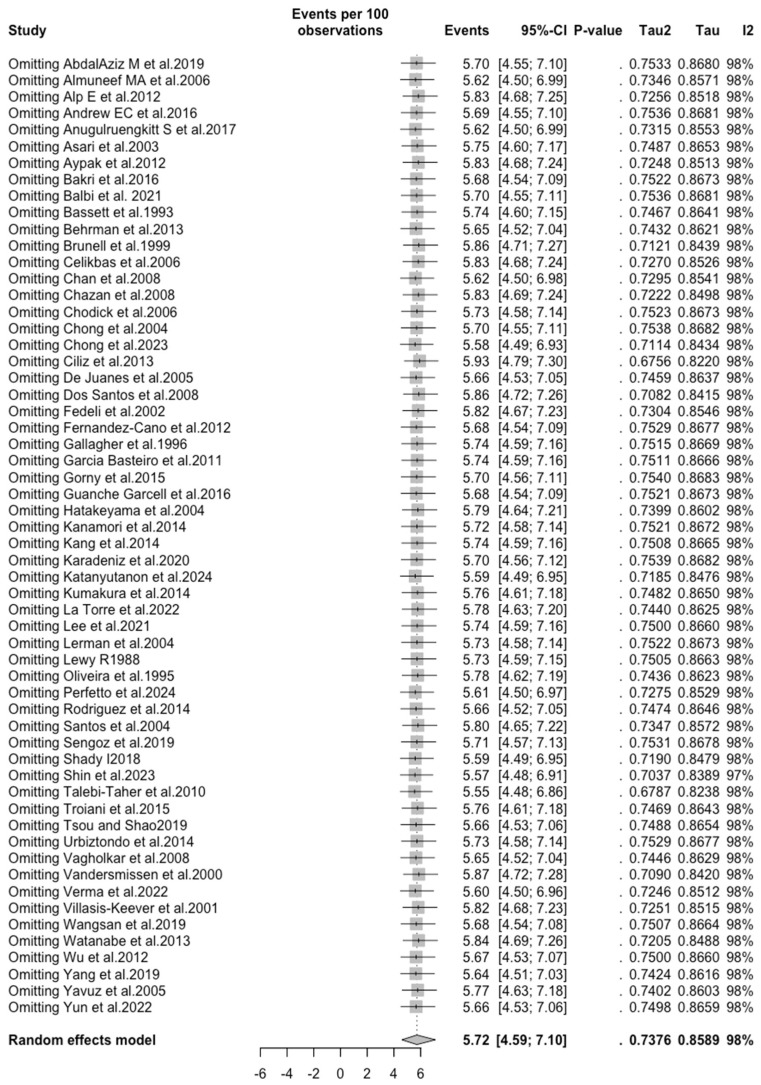
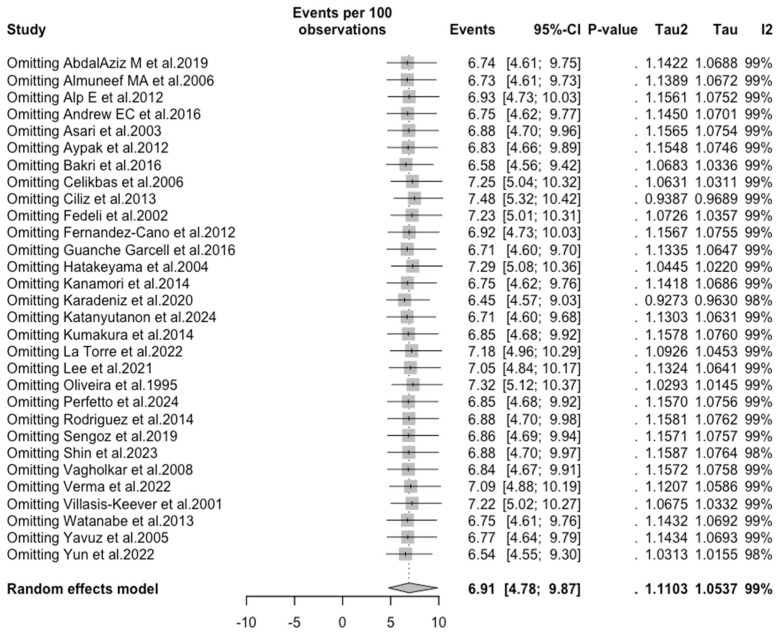
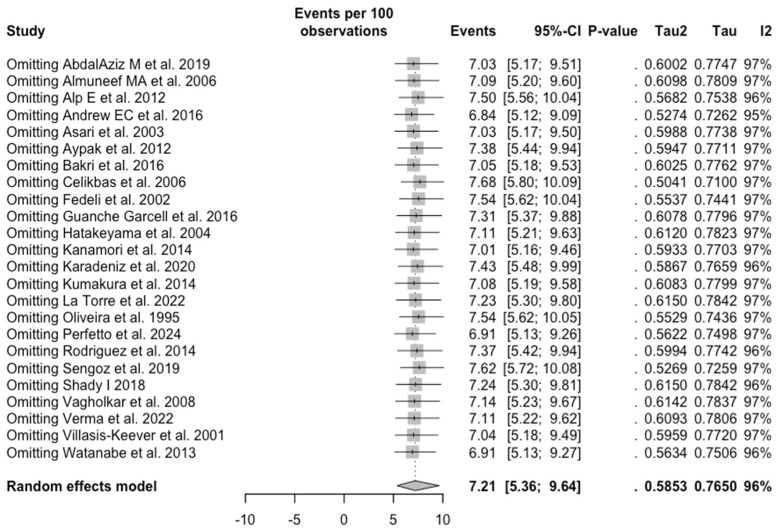
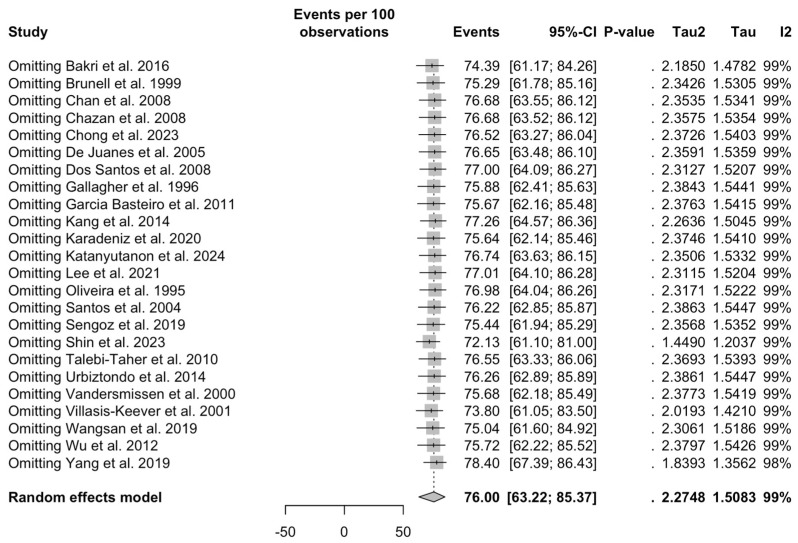
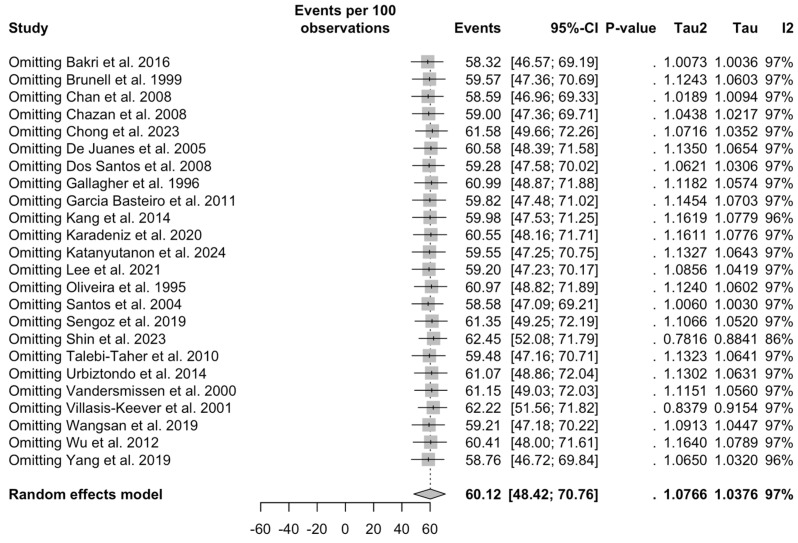
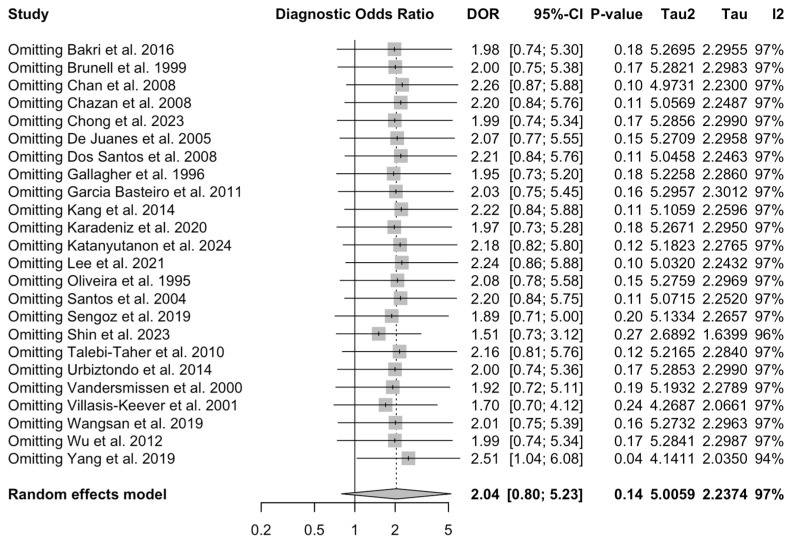
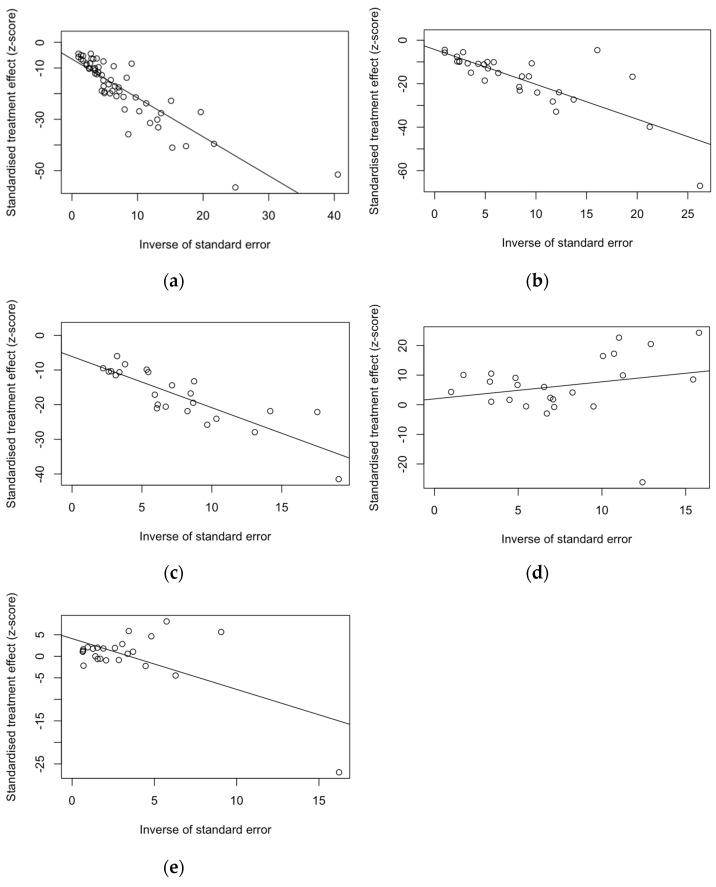
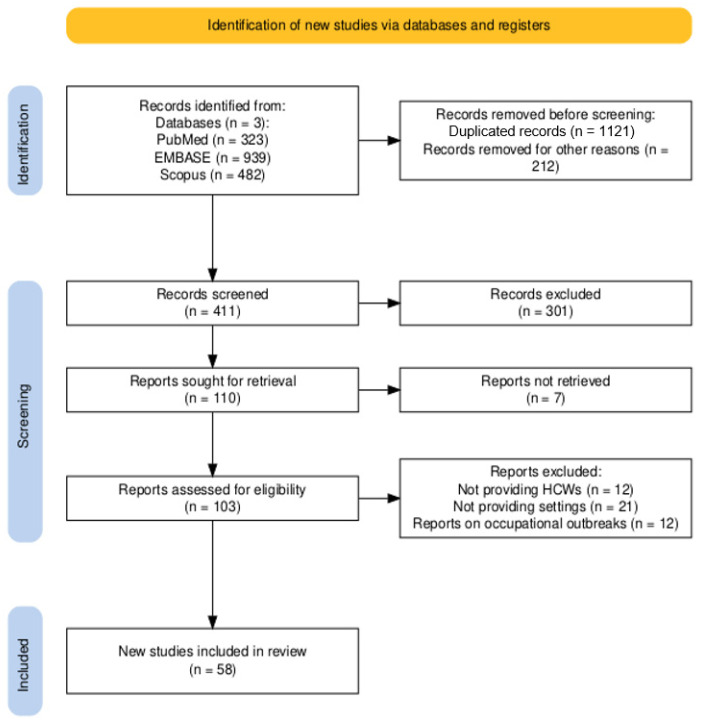
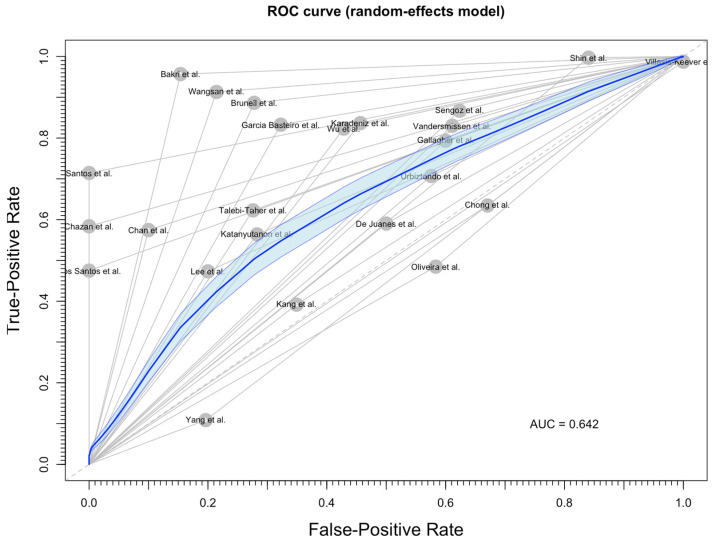
Healthcare workers (HCWs) are occupationally exposed to varicella zoster virus (VZV), and their inappropriate vaccination status could contribute to an outbreak involving both professionals and the patients they care for, with a potential impact on the general population. Therefore, since 2007, the Advisory Committee on Immunization Practices (ACIP) recommends that all HCWs have evidence of immunity against varicella. The present meta-analysis was therefore designed to collect the available evidence on the seronegative status of VZV among HCWs. PubMed, Scopus, and Embase databases were searched without backward limit for articles reporting on the seroprevalence of VZV among HCWs, and all articles meeting the inclusion criteria were included in a random-effect meta-analysis model. From 1744 initial entries, a total of 58 articles were included in the quantitative analysis (publication range: 1988 to 2024), for a pooled sample of 71,720 HCWs. Moreover, the included studies reported on seroprevalence data on measles (N = 36,043 HCWs) and rubella (N = 22,086 HCWs). Eventually, the pooled seronegative status for VZV was estimated to be 5.72% (95% confidence interval [95% CI] 4.59 to 7.10) compared to 6.91% (95% CI 4.79 to 9.87) for measles and 7.21% (5.36 to 9.64) for rubella, with a greater risk among subjects younger than 30 years at the time of the survey (risk ratio [RR] 1.434, 95% CI 1.172 to 1.756). Interestingly, medical history of either VZV infection/vaccination had low diagnostic performances (sensitivity 76.00%; specificity 60.12%; PPV of 96.12% but PNV of 18.64%). In summary, the available data suggest that newly hired HCWs are increasingly affected by low immunization rates for VZV but also for measles and rubella, stressing the importance of systematically testing test newly hired workers for all components of the measles-pertussis-rubella-varicella vaccine.
Keywords: chickenpox; healthcare workers; shingles; varicella zoster; varicella zoster vaccine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Rahaus M., Schünemann S., Wolff M.H. General Aspects Morphological and Biological Characteristics of Varicella-Zoster Virus. In: Wolff M., Schünemann S., Schmidt A., editors. Pathogenesis, and Clinical Aspects. Contrib Microbiol. Volume 3. Karger; Basel, Switzerland: 1999. pp. 1–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
