

The association between introduction of the micro-axial flow pump Impella in hospitals and in-hospital mortality in patients treated with extracorporeal membrane oxygenation: interrupted time-series analyses
- PMID: 39340610
- PMCID: PMC11438750
- DOI: 10.1186/s13613-024-01381-4
The association between introduction of the micro-axial flow pump Impella in hospitals and in-hospital mortality in patients treated with extracorporeal membrane oxygenation: interrupted time-series analyses
Abstract
Background: The micro-axial flow pump Impella, a new mechanical circulatory device for cardiogenic shock, is still only available in a limited number of hospitals, due to the facility certification requirements and insufficient evidence of the benefit of introducing Impella in hospitals. This study aimed to evaluate the impact of introducing Impella in hospitals on in-hospital mortality of patients treated with extracorporeal membrane oxygenation (ECMO).
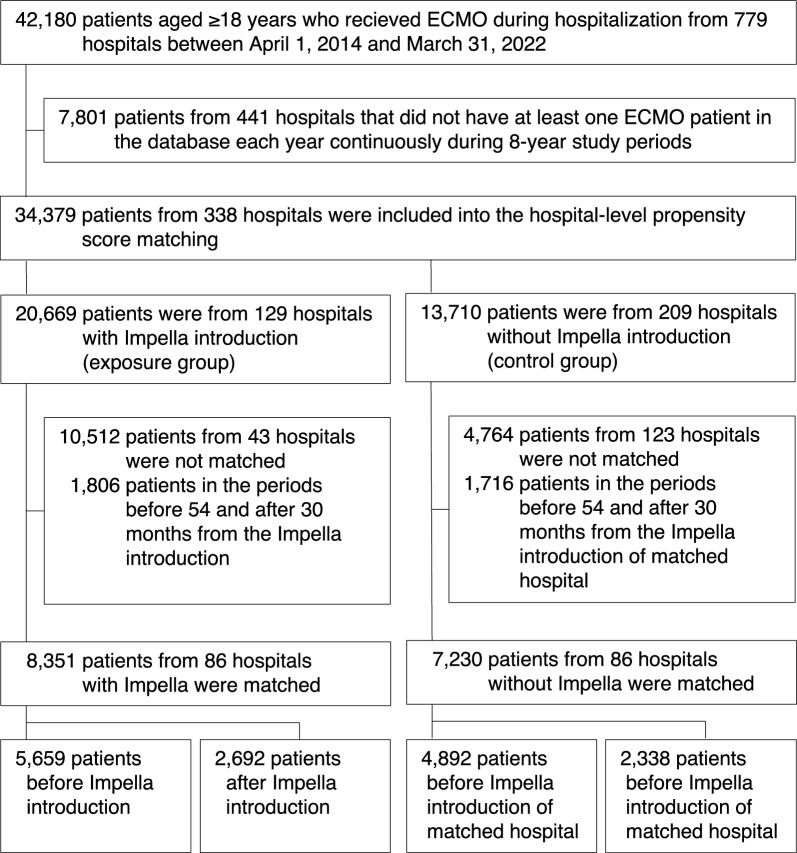
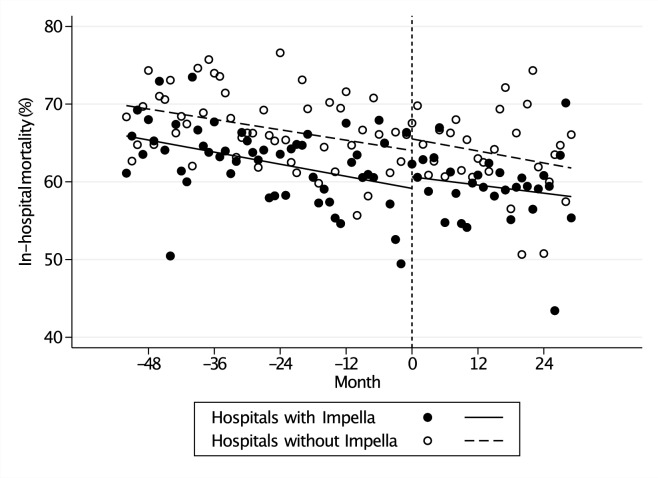
Methods: Using a nationwide Japanese inpatient database, we identified patients who received ECMO during hospitalization between 1 April 2014 and 31 March 2021. A hospital-level propensity score-matched cohort was created matching hospitals that introduced Impella (exposure group) to those that did not introduce Impella (control group). The inclusion period in each hospital was divided into two time periods according to the time of Impella introduction in the exposure group and the corresponding hospital in the control group (before and after exposure). The primary outcome was in-hospital mortality. Uncontrolled and controlled interrupted time-series analyses involved before-after exposure comparison and exposure-control comparison.
Results: Out of 34,379 eligible patients, we created a matched cohort of 8351 patients from 86 hospitals with Impella introduction (exposure group) and 7230 patients from 86 hospitals without Impella introduction (control group). In-hospital mortality before and after exposure was 62.5% and 59.3, respectively, in the exposure group; and 66.8% and 63.7%, respectively, in the control group. Uncontrolled interrupted time-series analysis showed no significant level change or trend change in the before-after exposure comparison in both the exposure and the control groups. Controlled interrupted time-series analysis also showed no significant level change (-0.01%; 95% confidence intervals -5.36% to + 5.33%) or trend change (+ 0.10%, -0.30% to + 0.40%) after exposure in the exposure-control comparison.
Conclusions: This nationwide inpatient database study showed no association between Impella introduction in hospitals and in-hospital mortality of patients who underwent ECMO. Because this study confined itself to analze of the impact of the introduction of Impella solely at the hospital level, further detailed studies are warranted to assess its efficacy at the patient level.
Keywords: Cost; Impella; Interrupted time series analysis; Micro-axial flow pump; Mortality; Venoarterial extracorporeal membrane oxygenation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Becher PM, Schrage B, Sinning CR, Schmack B, Fluschnik N, Schwarzl M, et al. Venoarterial extracorporeal membrane oxygenation for cardiopulmonary support. Circulation. 2018;138(20):2298–300. - PubMed
-
- Schrage B, Becher PM, Bernhardt A, Bezerra H, Blankenberg S, Brunner S, et al. Left ventricular unloading is associated with lower mortality in patients with cardiogenic shock treated with venoarterial extracorporeal membrane oxygenation: results from an international, multicenter cohort study. Circulation. 2020;142(22):2095–106. - PMC - PubMed
-
- Pappalardo F, Schulte C, Pieri M, Schrage B, Contri R, Soeffker G, et al. Concomitant implantation of Impella on top of veno-arterial extracorporeal membrane oxygenation may improve survival of patients with cardiogenic shock. Eur J Heart Fail. 2017;19:404–12. 10.1002/ejhf.668. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
