

Two distinct phenotypes of calcium oxalate stone formers could imply different long-term risks for renal function
- PMID: 39340639
- PMCID: PMC11449262
- DOI: 10.1007/s00240-024-01631-x
Two distinct phenotypes of calcium oxalate stone formers could imply different long-term risks for renal function
Abstract
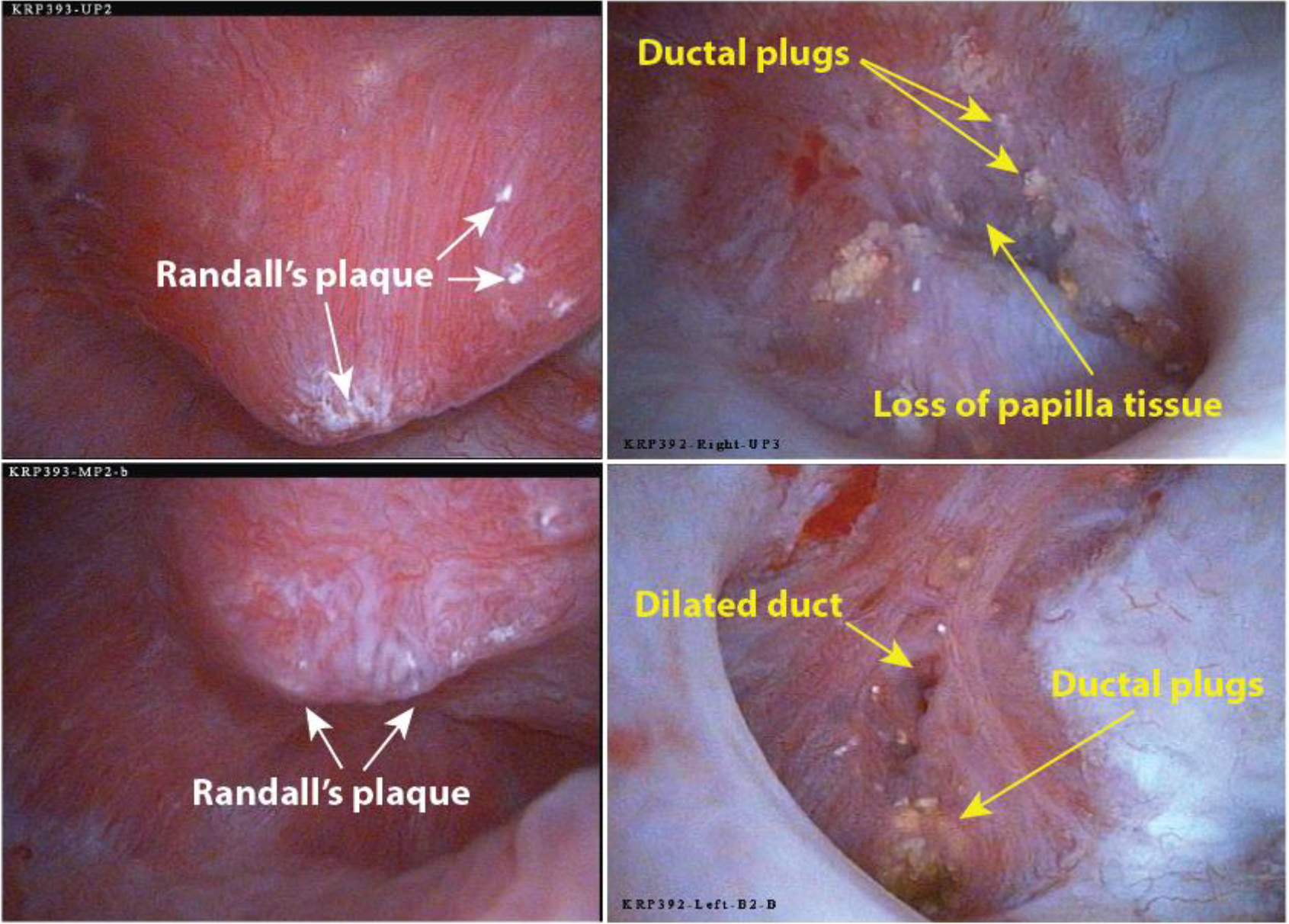
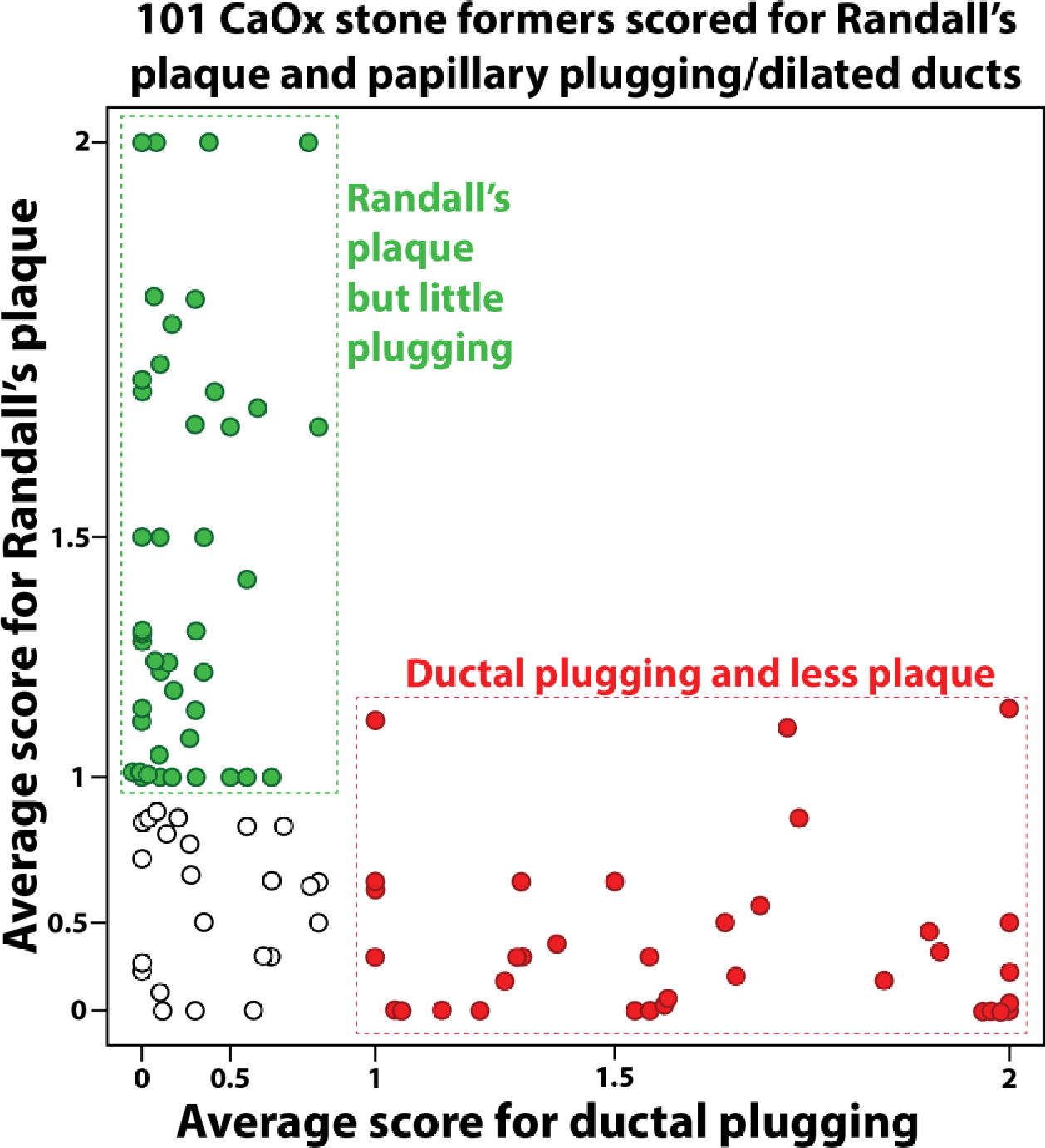
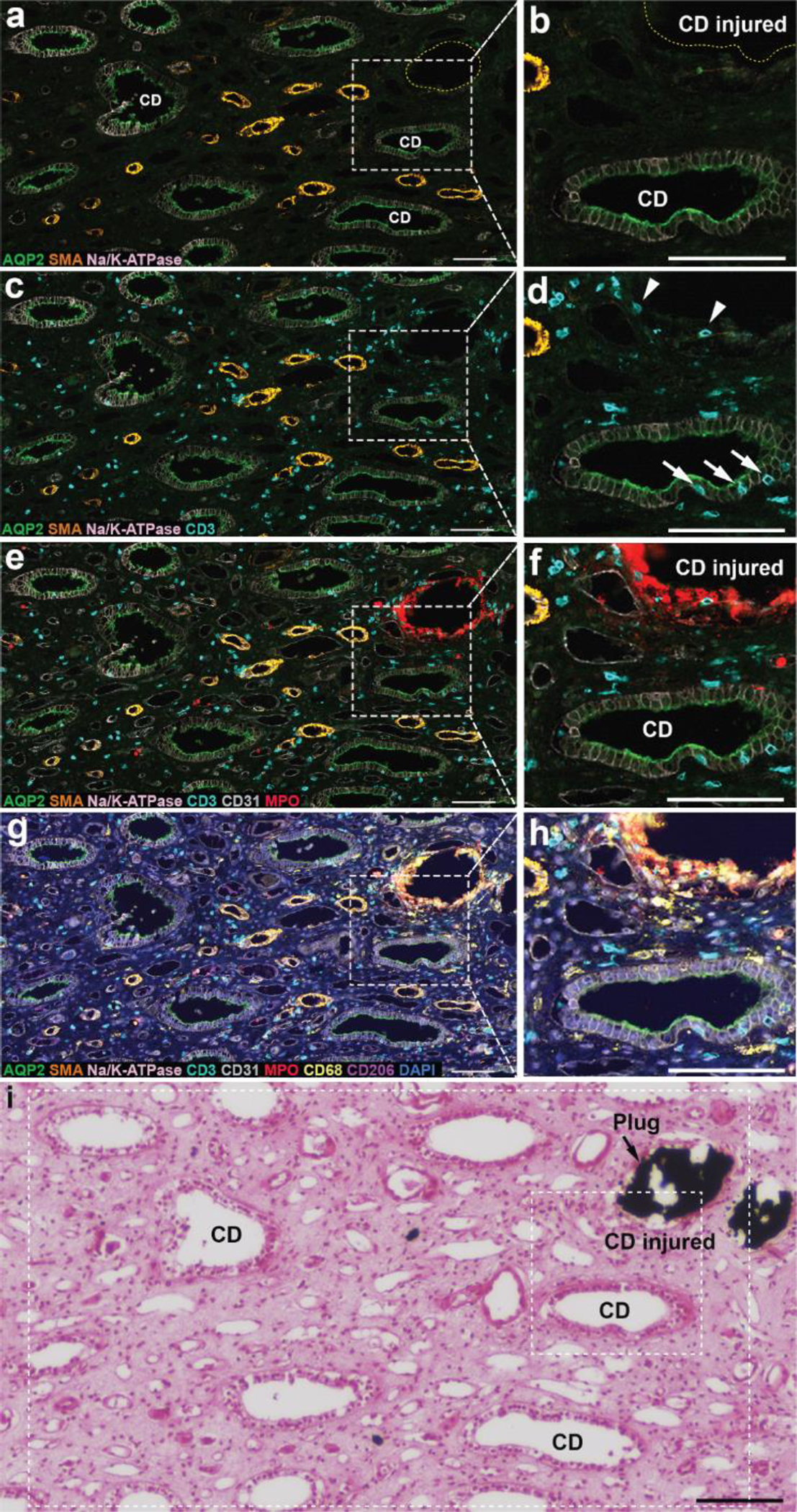
Endoscopic and biopsy findings have identified two distinct phenotypes among individuals with calcium oxalate (CaOx) kidney stones. The first type has normal renal papillae but shows interstitial mineral deposition, known as Randall's plaque. The other phenotype presents with collecting duct plugging and a higher incidence of loss of papilla tissue mass. With Randall's plaque, renal papilla injury involves the loss of small patches of calcified tissue (Randall's plaque detaching with the stone), which likely results in damage to only a few nephrons. In contrast, collecting duct mineral plugs are very large, causing obstruction to tubular flow. Since each terminal collecting duct drains thousands of nephrons, ductal plugs could lead to the degeneration of many nephrons and a significant loss of renal glomeruli. New visualization techniques for immune cells in papillary biopsies have revealed that the Randall's plaque phenotype is marked by the accumulation of macrophages around the plaque regions. In contrast, preliminary data on the plugging phenotype shows collecting duct damage with mineral plugs and increased T-lymphocytes throughout the papilla. These regions also show tubulitis, i.e., T-cell infiltration into nearby collecting duct epithelium. This suggests that while some CaOx stone formers may have some papillary inflammation but with minimal damage to nephrons, others suffer from obstruction to flow for many nephrons that may also include destructive inflammation in the renal tissue. We propose that CaOx stone formers with the plugging phenotype will have a higher long-term risk for loss of renal function.
Keywords: Calcium oxalate; Inflammation; Kidney stones; Nephrolithiasis.
© 2024. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Figures


Update of
-
Two distinct phenotypes of calcium oxalate stone formers could imply different long-term risks for renal function.Res Sq [Preprint]. 2024 Sep 2:rs.3.rs-4863593. doi: 10.21203/rs.3.rs-4863593/v1. Res Sq. 2024. Update in: Urolithiasis. 2024 Sep 28;52(1):133. doi: 10.1007/s00240-024-01631-x. PMID: 39281877 Free PMC article. Updated. Preprint.
References
-
- Roberson D, Sperling C, Shah A, Ziemba J (2020) Economic Considerations in the Management of Nephrolithiasis. Curr Urol Rep 21: 18. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
