

First interim results from FINE-REAL: a prospective, non-interventional, phase 4 study providing insights into the use and safety of finerenone in a routine clinical setting
- PMID: 39340711
- PMCID: PMC11649709
- DOI: 10.1007/s40620-024-02070-y
First interim results from FINE-REAL: a prospective, non-interventional, phase 4 study providing insights into the use and safety of finerenone in a routine clinical setting
Abstract
Background: Finerenone, a selective non-steroidal mineralocorticoid receptor antagonist, improves kidney and cardiovascular outcomes in patients with chronic kidney disease (CKD) associated with type 2 diabetes (T2D). The FINE-REAL study (NCT05348733) aims to evaluate the characteristics and treatment patterns of participants treated with finerenone in clinical practice.
Methods: FINE-REAL is a prospective, single-arm, non-interventional study of patients initiated on finerenone as part of their routine care in accordance with country-approved labels. The study, initiated in June 2022, is expected to be completed by January 2028. The cutoff for this pre-specified interim analysis was June 13, 2023.
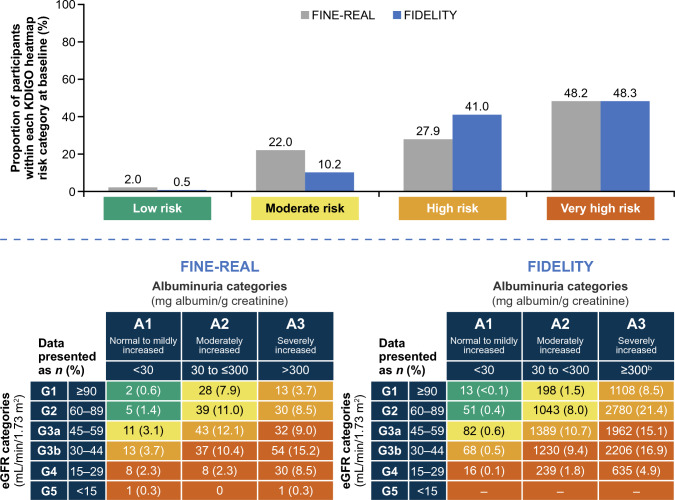
Results: Participants were recruited across nephrology, endocrinology, cardiology, and primary care settings. Of 556 participants enrolled in the study by the cut-off date, 504 were included in this analysis (median follow-up duration of 7 months [finerenone treatment initiation to last recorded observation]). At baseline, 76.1% of participants were in the high or very high (KDIGO) CKD risk categories. Angiotensin converting enzyme inhibitors/angiotensin receptor blockers and sodium-glucose cotransporter 2 inhibitors were prescribed to 71.8% and 46.6% of participants, respectively. Based on prescribing information, 87.9% and 12.1% of participants initiated finerenone at doses of 10 and 20 mg, respectively. Finerenone treatment was uninterrupted in 92.3% of participants after 7 months' median follow-up. Treatment-emergent adverse events occurred in 110 (21.8%) participants. Hyperkalemia occurred in 25 (5.0%) participants, with no cases leading to death, dialysis, or hospitalization.
Conclusion: At this interim analysis, finerenone was initiated in patients with CKD and T2D across various clinical practices participating in the study. Treatment discontinuation and hyperkalemia occurred infrequently.
Keywords: Chronic kidney disease; Finerenone; Non-interventional study; Type 2 diabetes.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: This study is sponsored by Bayer AG. The authors wrote the article with the assistance of a medical writer funded by the sponsor. The sponsor was involved in the study design and the writing of the report. Susanne B. Nicholas is supported by NIH research grants R01MD014712, RF00250-2022-0038, U2CDK129496, P50MD017366, and CDC project number 75D301-21-P-12254; received research support from Bayer AG for the submitted work, as well as research support from Goldfinch Bio, Travere, and Terasaki Institute of Biomedical Innovation; and personal fees and other support from AstraZeneca, Bayer AG, Gilead, Novo Nordisk, and Boehringer Ingelheim/Lilly. Ricardo Correa-Rotter has received consulting and/or speaker and/or advisory board fees and/or research support from AbbVie, AstraZeneca, Bayer, Boehringer Ingelheim, Chinook, Novo Nordisk and Roche. Nihar Desai works under contract with the Centers for Medicare and Medicaid Services to develop and maintain performance measures used for public reporting and pay for performance programs. He reports research grants and consulting for Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Cytokinetics, Merck, Novartis, SCPharmaceuticals, and Vifor. Lixin Guo has nothing to disclose. Sankar D. Navaneethan reports receipt of personal fees from AstraZeneca (Data and Safety Monitoring Board), ACI clinical (Clinical Event Committee), Bayer, Boehringer Ingelheim/Lilly, GSK, Intercept, Vifor, and Vertex; and grants from Keryx outside the submitted work. Kevin M. Pantalone discloses speaker bureau fees from AstraZeneca, Corcept Therapeutics, Merck, and Novo Nordisk; consulting fees from AstraZeneca, Bayer, Corcept Therapeutics, Diasome, Eli Lilly, Novo Nordisk, Merck, Sanofi, and Twinhealth; and research support from Bayer, Novo Nordisk, Merck, and Twinhealth. Christoph Wanner reports steering committee and advisory board participation as well as lecturing honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, FMC, Gilead, GSK, MSD, Sanofi, and Vifor. Stefanie Hamacher was an employee of ClinStat GmbH at the time of the study and reports consulting or advisory roles of her former CRO with Bayer AG. Samuel Fatoba is an employee of Bayer U.S. LLC, Pharmaceuticals. Andrea Horvat-Broecker is an employee of Bayer AG, Germany. Antonio Garreta-Rufas is an employee of Bayer AG, Germany. Alain Gay was an employee of Bayer AG, Germany at the time the interim analysis was performed. Martin Merz is an employee of Bayer AG, Germany. David C. Wheeler has received honoraria from Astellas, AstraZeneca (ongoing consultancy agreement), Amgen, Bayer, Boehringer Ingelheim, GSK, Gilead, Janssen, Mundipharma, Merck Sharp and Dohme, Tricida, Vifor, and Zydus. Ethical approval: Documented approval from appropriate independent ethics committees/institutional review boards was obtained for all participating centers in applicable countries prior to study start. The study is being conducted within an approved drug indication in accordance with guidelines and regulations of the European Medicines Agency, the U.S. Food and Drug Administration [15, 16], and applicable local laws and regulations. Human and animal rights: Documented approval from appropriate independent ethics committees/institutional review boards was obtained for all participating centers in applicable countries prior to study start. The study is being conducted within an approved drug indication in accordance with guidelines and regulations of the European Medicines Agency, the U.S. Food and Drug Administration, and applicable local laws and regulations. All participants provided written informed consent. This article does not contain any studies with animals performed by any of the authors. Informed consent to participate: All participants provided written informed consent.
Figures
References
-
- IDF. IDF diabetes atlas. 2021. https://diabetesatlas.org/. Accessed 3 May 2022.
-
- ISN. ISN global kidney health atlas. 2023. https://www.theisn.org/wp-content/uploads/media/ISN%20Atlas_2023%20Digit.... Accessed 23 November 2023.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
