

Insulin resistance assessed by estimated glucose disposal rate and risk of atherosclerotic cardiovascular diseases incidence: the multi-ethnic study of atherosclerosis
- PMID: 39342205
- PMCID: PMC11439291
- DOI: 10.1186/s12933-024-02437-2
Insulin resistance assessed by estimated glucose disposal rate and risk of atherosclerotic cardiovascular diseases incidence: the multi-ethnic study of atherosclerosis
Abstract
Background: To investigate the relationship between estimated glucose disposal rate (eGDR), a surrogate indicator of insulin resistance, and atherosclerotic cardiovascular diseases (ASCVD) incidence risk.
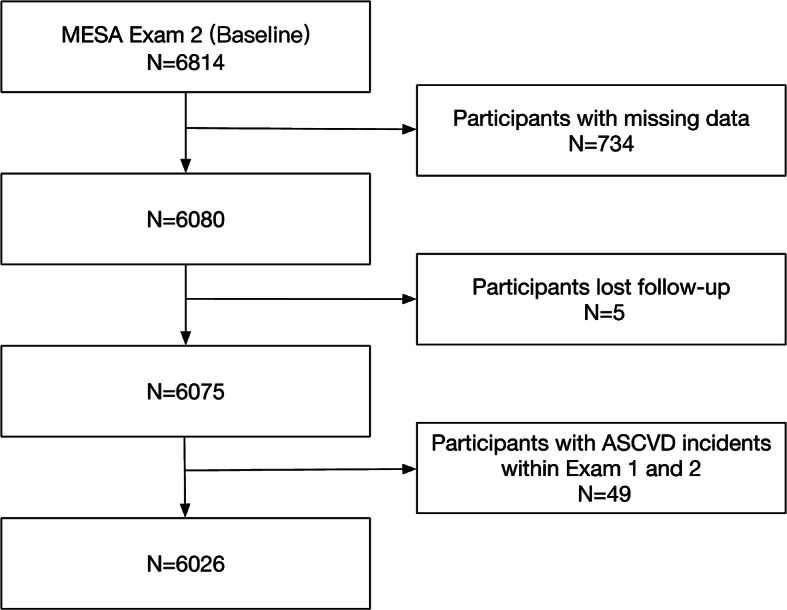
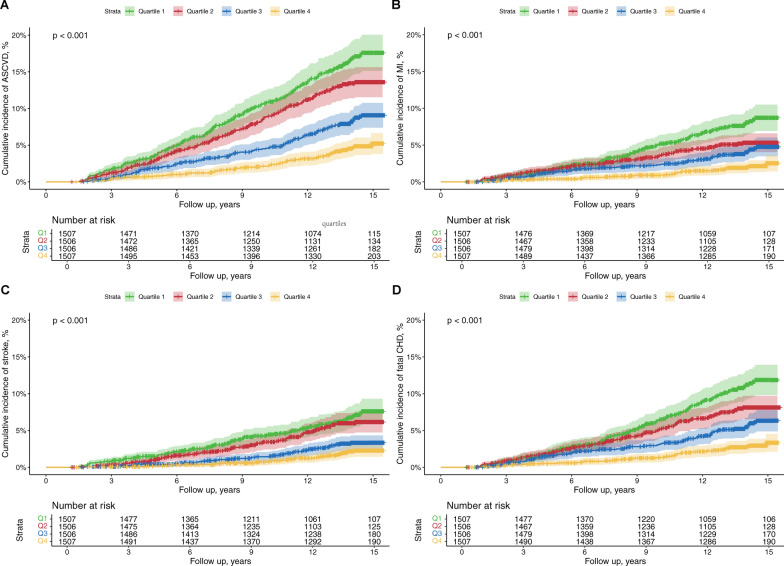
Methods: This prospective cohort study utilized data from the 6026 participants from the Multi-Ethnic Study of Atherosclerosis. The eGDR (mg/kg/min) was computed as 21.158 - (0.09 × waist circumference [cm]) - (3.407 × hypertension [yes/no]) - (0.551 × HbA1c [%]). The population was categorized into four subgroups according to the quartiles (Q) of eGDR. Cox proportional hazard models were applied to assess the associations between eGDR and ASCVD incidence, and restricted cubic spine (RCS) was employed to examine the dose-response relationship.
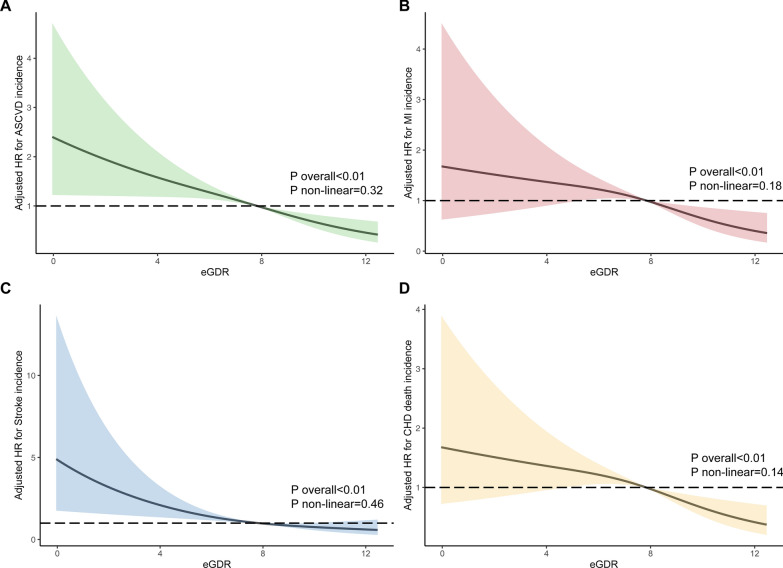
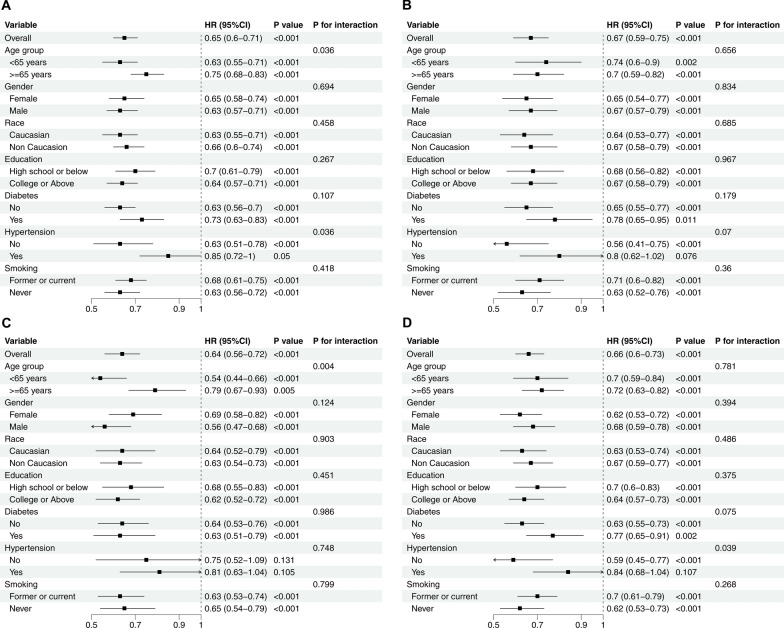
Results: The mean age of participants was 63.6 ± 10.1 years, comprising 3163 (52.5%) women. Over a median follow-up duration of 14.1 years, 565 (9.4%) developed ASCVD, including 256 (4.2%) myocardial infarctions, 234 (3.9%) strokes, and 358 (5.9%) fatal coronary heart disease. Compared to the lowest quartile, the adjusted hazard ratios (95% confidence intervals) for incident ASCVD for Q2-Q4 were 0.87 (0.68-1.10), 0.63 (0.47-0.84), and 0.43 (0.30-0.64), respectively. Per 1 standard deviation increase in eGDR was associated with a 30% (HR: 0.70, 95% CI 0.60-0.80) risk reduction of ASCVD, with the subgroup analyses indicating that age and hypertension modified the association (P for interaction < 0.05). RCS analysis indicated a significant and linear relationship between eGDR and ASCVD incidence risk.
Conclusion: eGDR level was negatively associated with incident ASCVD risk in a linear fashion among the general population. Our findings may contribute to preventive measures by improving ASCVD risk assessment.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, Briggs AM. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–858. 10.1016/s0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- Ferrari AJ, Santomauro DF, Aali A, Abate YH, Abbafati C, Abbastabar H, Bell ML. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2133–61. 10.1016/s0140-6736(24)00757-8. - DOI - PMC - PubMed
-
- Naghavi M, Ong KL, Aali A, Ababneh HS, Abate YH, Abbafati C, Alqutaibi AY. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2100–32. 10.1016/s0140-6736(24)00367-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
