

Association of diaphragmatic dysfunction with duration of mechanical ventilation in patients in the pediatric intensive care unit: a prospective cohort study
- PMID: 39342241
- PMCID: PMC11438377
- DOI: 10.1186/s12887-024-05092-4
Association of diaphragmatic dysfunction with duration of mechanical ventilation in patients in the pediatric intensive care unit: a prospective cohort study
Abstract
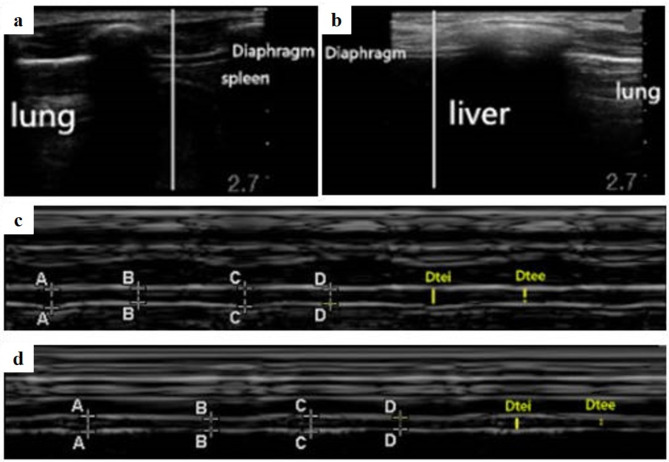
Background: Mechanical ventilation (MV) can cause diaphragmatic injury and ventilator induced diaphragmatic dysfunction (VIDD). Diaphragm ultrasonography (DU) is increasingly used to assess diaphragmatic anatomy, function and pathology of patients receiving MV in the pediatric intensive care unit (PICU). We report the poor contractile ability of diaphragm during ventilation of critically ill patients in our PICU and the association to prolonged length of MV and PICU stay.
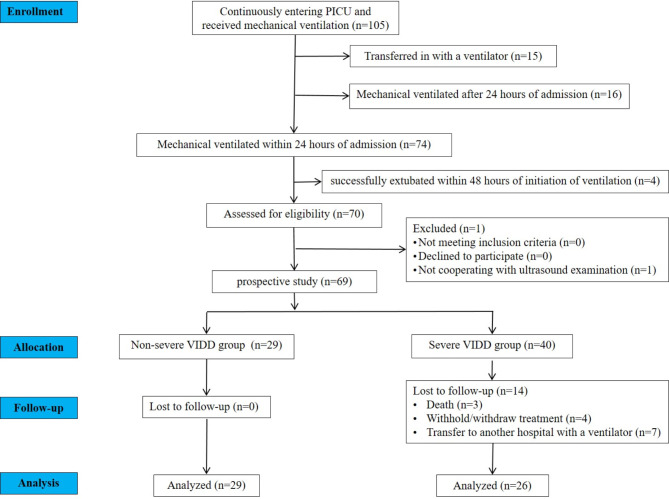
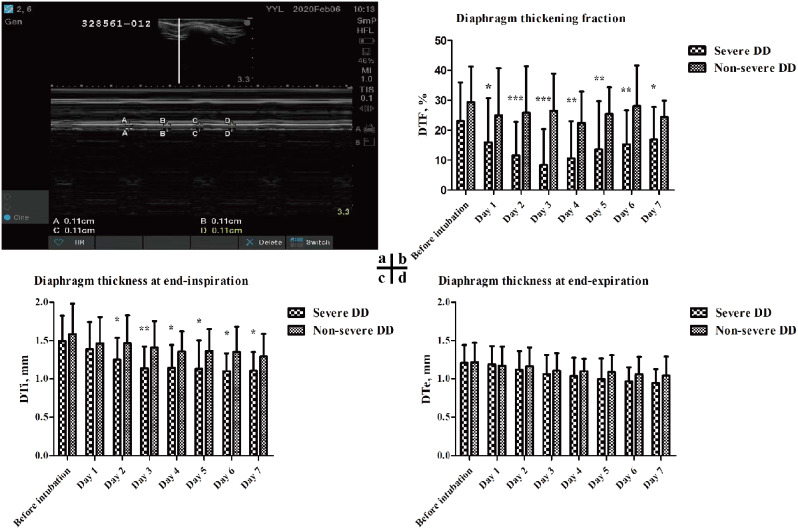
Methods: Patients who received MV within 24 h of admission to the PICU, expected to undergo continuous MV for more than 48 h and succeeded to extubate were included in the study. DU monitoring was performed daily after the initiation of MV until extubation. Diaphragm thickening fraction (DTF) measured by DU was used as an indicator of diaphragmatic contractile activity. Patients with bilateral DTF = 0% during DU assessment were allocated into the severe VIDD group (n = 26) and the rest were into non-severe VIDD group (n = 29). The association of severe VIDD with individual length of MV, hospitalization and PICU stay were analyzed.
Results: With daily DU assessment, severe VIDD occurred on 2.9 ± 1.2 days after the initiation of MV, and lasted for 1.9 ± 1.7 days. Values of DTF of all patients recovered to > 10% before extubation. The severe VIDD group had a significantly longer duration (days) of MV [12.0 (8.0-19.3) vs. 5.0 (3.5-7.5), p < 0.001] and PICU stay (days) [30.5 (14.9-44.5) vs. 13.0 (7.0-24.5), p < 0.001]. The occurrence of severe VIDD, first day of severe VIDD and length of severe VIDD were significantly positively associated with the duration of MV and PICU stay. The occurrence of severe VIDD on the second and third days after initiation of MV significantly associated to longer PICU stay (days) [43.0 (9.0-70.0) vs. 13.0 (3.0-40.0), p = 0.009; 36.0 (17.0-208.0) vs. 13.0 (3.0-40.0), p = 0.005, respectively], and the length of MV (days) was significantly longer in those with severe VIDD on the third day after initiation of MV [16.5 (7.0-29.0) vs. 5.0 (2.0-22.0), p = 0.003].
Conclusions: Daily monitoring of diaphragmatic function with bedside ultrasonography after initiation of MV is necessary in critically ill patients in PICU and the influences and risk factors of severe VIDD need to be further studied. (355 words).
Keywords: Diaphragm thickening fraction; Diaphragmatic ultrasound; Pediatric critical care; Ventilator induced diaphragmatic dysfunction.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Temporary transvenous diaphragm pacing vs. standard of care for weaning from mechanical ventilation: study protocol for a randomized trial.Trials. 2019 Jan 17;20(1):60. doi: 10.1186/s13063-018-3171-9. Trials. 2019. PMID: 30654837 Free PMC article.
-
Early rehabilitation relieves diaphragm dysfunction induced by prolonged mechanical ventilation: a randomised control study.BMC Pulm Med. 2021 Mar 29;21(1):106. doi: 10.1186/s12890-021-01461-2. BMC Pulm Med. 2021. PMID: 33781259 Free PMC article. Clinical Trial.
-
Hydrogen sulfide donor protects against mechanical ventilation-induced atrophy and contractile dysfunction in the rat diaphragm.Clin Transl Sci. 2021 Nov;14(6):2139-2145. doi: 10.1111/cts.13081. Epub 2021 Jun 16. Clin Transl Sci. 2021. PMID: 34080307 Free PMC article.
-
Outcomes in critically ill patients after diaphragmatic stimulation on ventilator-induced diaphragmatic dysfunction: a systematic review.Eur J Phys Rehabil Med. 2023 Dec;59(6):772-781. doi: 10.23736/S1973-9087.23.08031-0. Eur J Phys Rehabil Med. 2023. PMID: 38214045 Free PMC article.
-
Clinical review: ventilator-induced diaphragmatic dysfunction--human studies confirm animal model findings!Crit Care. 2011 Mar 11;15(2):206. doi: 10.1186/cc10023. Crit Care. 2011. PMID: 21457528 Free PMC article. Review.
Cited by
-
Serial sonographic assessment of diaphragmatic atrophy and lung injury patterns in mechanically ventilated preterm infants to predict extubation failure: a prospective observational study.Eur J Pediatr. 2024 Dec 18;184(1):90. doi: 10.1007/s00431-024-05927-3. Eur J Pediatr. 2024. PMID: 39692861
References
-
- Hannan LM, De Losa R, Romeo N, Muruganandan S. Diaphragm dysfunction: a comprehensive review from diagnosis to management. Intern Med J. 2022;52(12):2034–45. - PubMed
-
- Egbuta C, Easley RB. Update on ventilation management in the Pediatric Intensive Care Unit. Paediatr Anaesth. 2022;32(2):354–62. - PubMed
-
- Kim WY, Suh HJ, Hong SB, Koh Y, Lim CM. Diaphragm dysfunction assessed by ultrasonography: influence on weaning from mechanical ventilation. Crit Care Med. 2011;39(12):2627–30. - PubMed
-
- Goligher EC, Brochard LJ, Reid WD, Fan E, Saarela O, Slutsky AS, et al. Diaphragmatic myotrauma: a mediator of prolonged ventilation and poor patient outcomes in acute respiratory failure. Lancet Respir Med. 2019;7(1):90–8. - PubMed
-
- Dres M, Dubé BP, Mayaux J, Delemazure J, Reuter D, Brochard L, et al. Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am J Respir Crit Care Med. 2017;195(1):57–66. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
