

Effects of white matter hyperintensity burden on functional outcome after mild versus moderate-to-severe ischemic stroke
- PMID: 39343768
- PMCID: PMC11439954
- DOI: 10.1038/s41598-024-71936-9
Effects of white matter hyperintensity burden on functional outcome after mild versus moderate-to-severe ischemic stroke
Abstract
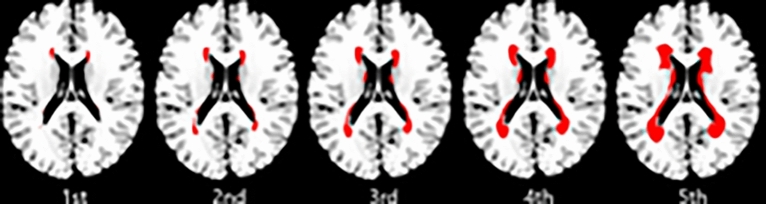
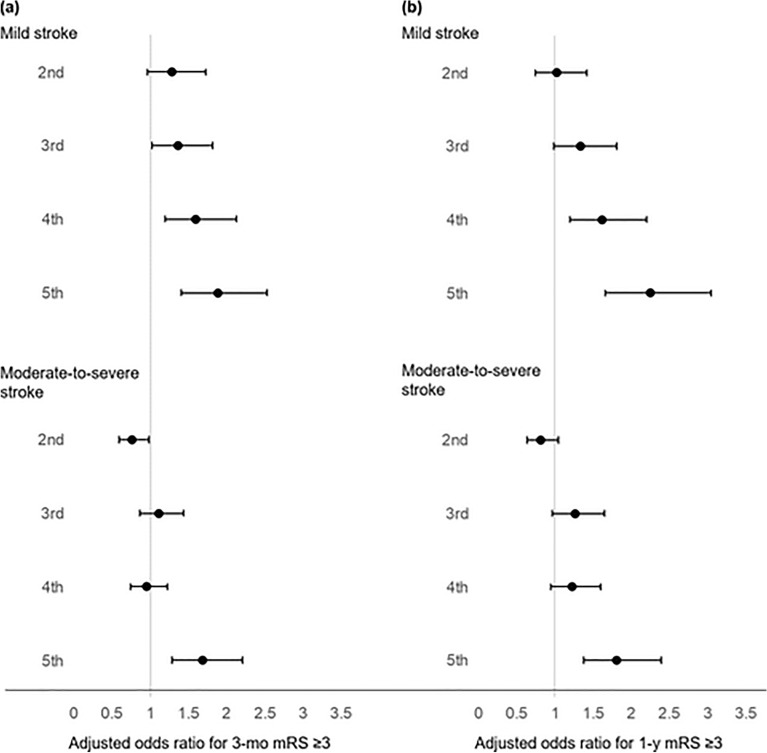
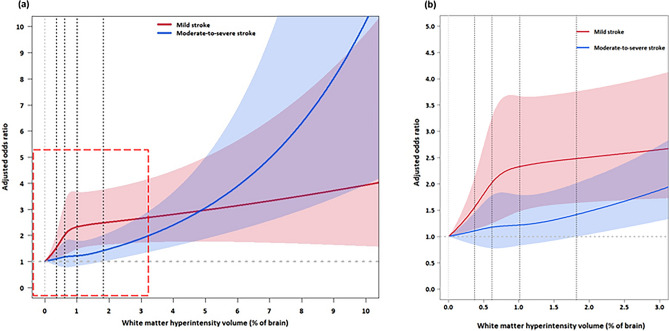
It is uncertain whether the prognostic power of white matter hyperintensity (WMH) on post-stroke outcomes is modulated as a function of initial neurological severity, a critical determinant of outcome after stroke. This multi-center MRI study tested if higher WMH quintiles were associated with 3-month poor functional outcome (modified Rankin Scale ≥ 3) for mild versus moderate-to-severe ischemic stroke. Mild and moderate-to-severe stroke were defined as admission National Institute of Health Stroke Scale scores of 1-4 and ≥ 5, respectively. Mean age of the enrolled patients (n = 8918) was 67.2 ± 12.6 years and 60.1% male. The association between WMH quintiles and poor functional outcome was modified by stroke severity (p-for-interaction = 0.008). In mild stroke (n = 4994), WMH quintiles associated with the 3-month outcome in a dose-dependent manner for the 2nd to 5th quintile versus the 1st quintile, with adjusted-odds-ratios (aOR [95% confidence interval]) being 1.29 [0.96-1.73], 1.37 [1.02-1.82], 1.60 [1.19-2.13], and 1.89 [1.41-2.53], respectively. In moderate-to-severe stroke (n = 3924), however, there seemed to be a threshold effect: only the highest versus the lowest WMH quintile was significantly associated with poor functional outcome (aOR 1.69 [1.29-2.21]). WMH burden aggravates 3-month functional outcome after mild stroke, but has a lesser modulatory effect for moderate-to-severe stroke, likely due to saturation effects.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
