

Advances in Understanding Hepatocellular Carcinoma Vasculature: Implications for Diagnosis, Prognostication, and Treatment
- PMID: 39344546
- PMCID: PMC11444852
- DOI: 10.3348/kjr.2024.0307
Advances in Understanding Hepatocellular Carcinoma Vasculature: Implications for Diagnosis, Prognostication, and Treatment
Abstract
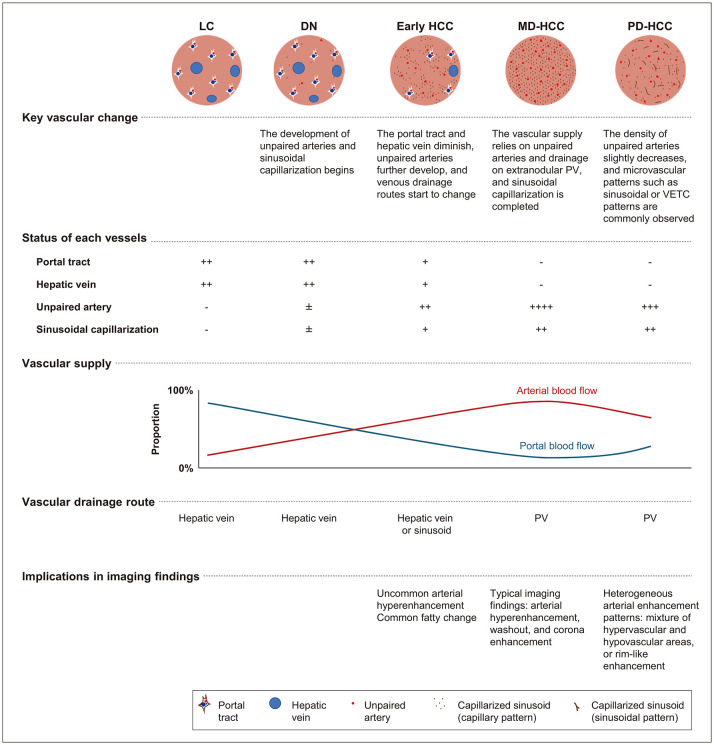
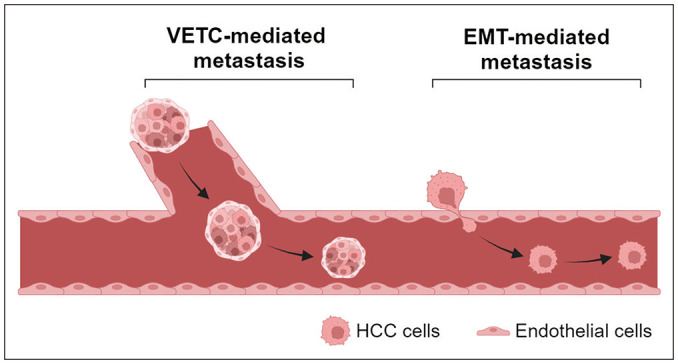
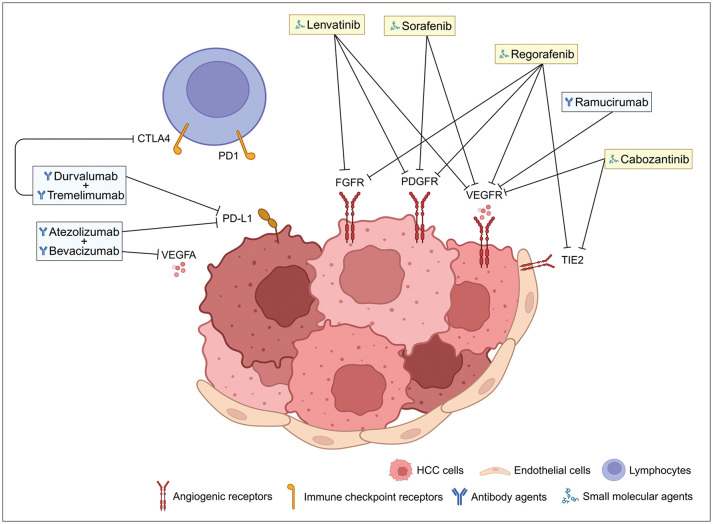
Hepatocellular carcinoma (HCC) progresses through multiple stages of hepatocarcinogenesis, with each stage characterized by specific changes in vascular supply, drainage, and microvascular structure. These vascular changes significantly influence the imaging findings of HCC, enabling non-invasive diagnosis. Vascular changes in HCC are closely related to aggressive histological characteristics and treatment responses. Venous drainage from the tumor toward the portal vein in the surrounding liver facilitates vascular invasion, and the unique microvascular pattern of vessels that encapsulate the tumor cluster (known as a VETC pattern) promotes vascular invasion and metastasis. Systemic treatments for HCC, which are increasingly being used, primarily target angiogenesis and immune checkpoint pathways, which are closely intertwined. By understanding the complex relationship between histopathological vascular changes in hepatocarcinogenesis and their implications for imaging findings, radiologists can enhance the accuracy of imaging diagnosis and improve the prediction of prognosis and treatment response. This, in turn, will ultimately lead to better patient care.
Keywords: Angiogenesis; Hepatocarcinogenesis; Hepatocellular carcinoma; Systemic therapy; Vascular invasion.
Copyright © 2024 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Rumgay H, Ferlay J, de Martel C, Georges D, Ibrahim AS, Zheng R, et al. Global, regional and national burden of primary liver cancer by subtype. Eur J Cancer. 2022;161:108–118. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
