

Cardiomyopathy-Associated Chronic Heart Failure in Infants Aged <1 Year: A Prospective Observational Cohort Over 5 Years in Northern China
- PMID: 39344650
- PMCID: PMC11681489
- DOI: 10.1161/JAHA.122.029121
Cardiomyopathy-Associated Chronic Heart Failure in Infants Aged <1 Year: A Prospective Observational Cohort Over 5 Years in Northern China
Abstract
Background: There have been few large-scale studies on the outcomes of cardiomyopathy-associated heart failure (HF) in infants aged <1 year. This study aimed to assess longitudinal echocardiographic outcomes of infants with HF secondary to cardiomyopathy who survived for >1 year.
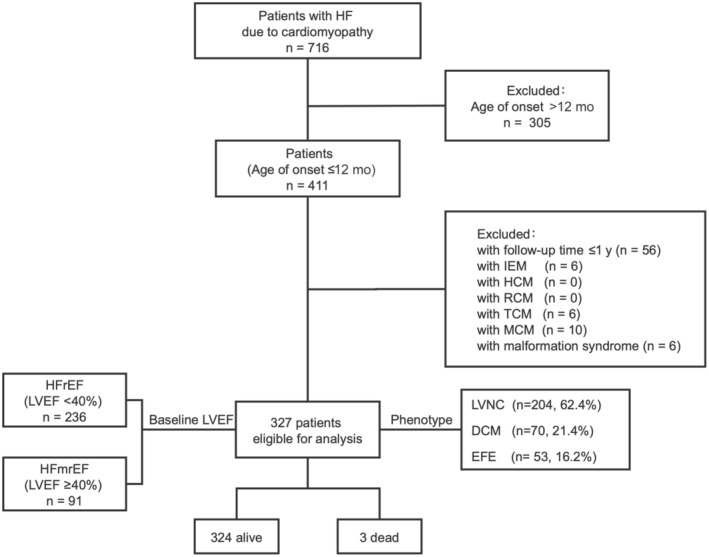
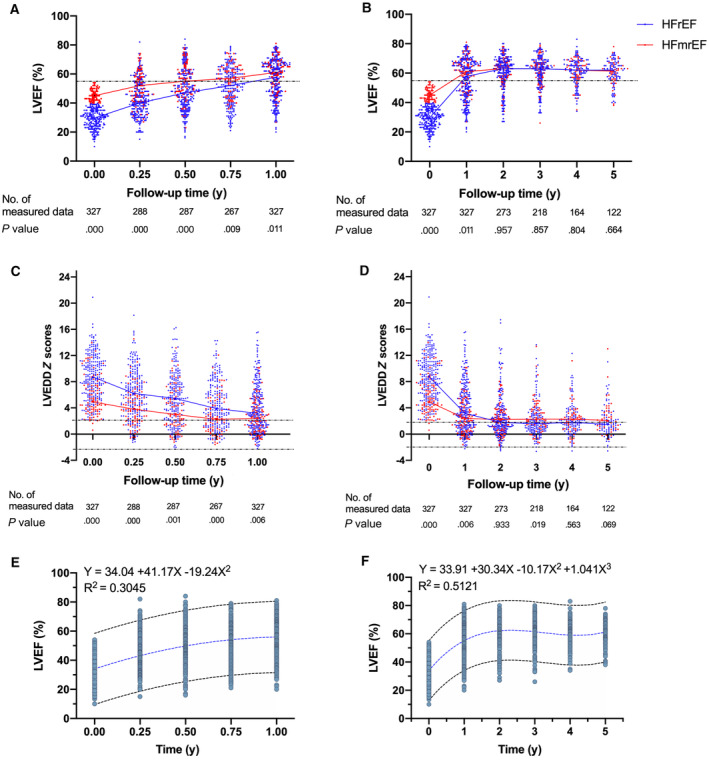
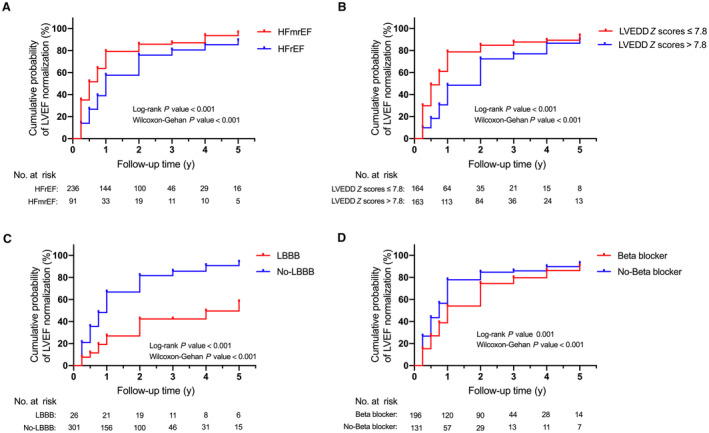
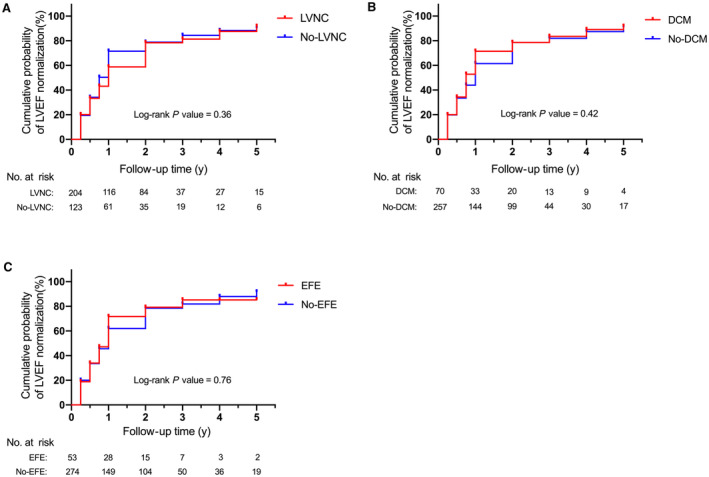
Methods and results: A prospective observational study following 327 infant patients up to 5 years in 2 large pediatric heart centers in Northern China between January 2010 and December 2018. A total of 236 (72.2%) patients had reduced left ventricular ejection fraction (LVEF) (HF with reduced ejection fraction group; LVEF <40%), 91 (27.8%) patients had midrange LVEF (HF with midrange ejection fraction group; LVEF ≥40% but <55%). LVEF improved significantly within the first year and remained stable in years 2 through 5 for both groups. The HF with midrange ejection fraction group had a higher rate of LVEF normalization (hazard ratio, 1.65; P<0.001). Baseline LVEF ≥40%, baseline left ventricular end-diastolic diameter Z score <7.8, the absence of left bundle-branch block, and the absence of β-blocker use were 4 independent favorable predictors for future LVEF normalization. A total of 62.4% of enrolled patients were diagnosed with left ventricular noncompaction. No significant difference in LVEF normalization was found among the different types of cardiomyopathy studied.
Conclusions: A significant number of infants with cardiomyopathy who survived >1 year were found to improve with medical therapies during the first year of diagnosis. Poorer outcomes were associated with decreased LVEF and increased heart size at diagnosis baseline, the presence of left bundle-branch block and use of β blockers. The Northern Chinese pediatric population may have a high proportion of left ventricular noncompaction.
Keywords: cardiomyopathy; echocardiography; heart failure; longitudinal; pediatrics.
Figures
Similar articles
-
Characteristics, Outcomes, and Treatment of Heart Failure With Improved Ejection Fraction.J Am Heart Assoc. 2019 Mar 19;8(6):e011077. doi: 10.1161/JAHA.118.011077. J Am Heart Assoc. 2019. PMID: 30845873 Free PMC article.
-
Association of Prior Left Ventricular Ejection Fraction With Clinical Outcomes in Patients With Heart Failure With Midrange Ejection Fraction.JAMA Cardiol. 2020 Sep 1;5(9):1027-1035. doi: 10.1001/jamacardio.2020.2081. JAMA Cardiol. 2020. PMID: 32936274 Free PMC article.
-
Trajectories of Left Ventricular Ejection Fraction After Acute Decompensation for Systolic Heart Failure: Concomitant Echocardiographic and Systemic Changes, Predictors, and Impact on Clinical Outcomes.J Am Heart Assoc. 2021 Feb 2;10(3):e017822. doi: 10.1161/JAHA.120.017822. Epub 2021 Jan 26. J Am Heart Assoc. 2021. PMID: 33496189 Free PMC article.
-
Quality of life in patients with heart failure and improved ejection fraction: one-year changes and prognosis.ESC Heart Fail. 2022 Dec;9(6):3804-3813. doi: 10.1002/ehf2.14098. Epub 2022 Aug 2. ESC Heart Fail. 2022. PMID: 35916351 Free PMC article. Review.
-
Point-of-care ultrasound to assess left ventricular ejection fraction in heart failure in unselected patients in primary care: a systematic review.Fam Pract. 2025 Feb 7;42(2):cmae040. doi: 10.1093/fampra/cmae040. Fam Pract. 2025. PMID: 39162139
References
-
- Kantor PF, Lougheed J, Dancea A, McGillion M, Barbosa N, Chan C, Dillenburg R, Atallah J, Buchholz H, Chant‐Gambacort C, et al. Presentation, diagnosis, and medical management of heart failure in children: Canadian Cardiovascular Society guidelines. Can J Cardiol. 2013;29:1535–1552. doi: 10.1016/j.cjca.2013.08.008 - DOI - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, Gonzalez‐Juanatey JR, Harjola VP, Jankowska EA, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Rev Esp Cardiol (Engl ed). 2016;69:1167. - PubMed
-
- Alexander PM, Daubeney PE, Nugent AW, Lee KJ, Turner C, Colan SD, Robertson T, Davis AM, Ramsay J, Justo R, et al. Long‐term outcomes of dilated cardiomyopathy diagnosed during childhood: results from a national population‐based study of childhood cardiomyopathy. Circulation. 2013;128:2039–2046. doi: 10.1161/CIRCULATIONAHA.113.002767 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
