

Circulating Plasma Proteins in Aortic Stenosis: Associations With Severity, Myocardial Response, and Clinical Outcomes
- PMID: 39344657
- PMCID: PMC11681473
- DOI: 10.1161/JAHA.124.035486
Circulating Plasma Proteins in Aortic Stenosis: Associations With Severity, Myocardial Response, and Clinical Outcomes
Abstract
Background: Echocardiographic indexes of aortic stenosis may not comprehensively reflect disease morbidity. Plasma proteomic profiling may add prognostic value in these patients.
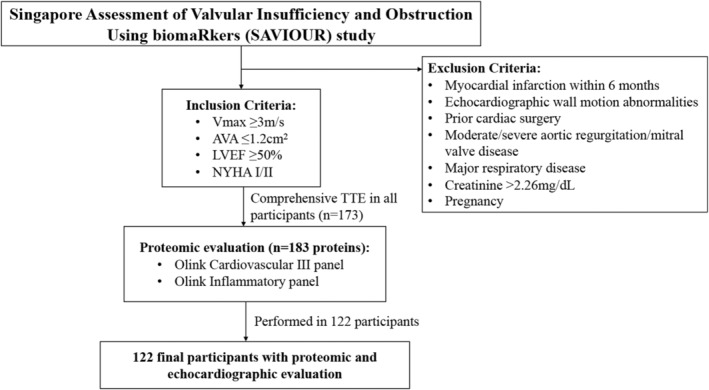
Methods and results: Proximity extension assays (Olink) of 183 circulating cardiovascular and inflammatory proteins were performed in a prospective follow-up study of 122 asymptomatic/minimally symptomatic patients (mean±SD age, 69.1±10.9 years; 61% men) with moderate to severe aortic stenosis and preserved left ventricular ejection fraction. Protein signatures of higher-risk echocardiographic subgroups were determined. Associations of proteins with the primary composite outcome (heart failure hospitalization, progression to New York Heart Association class III-IV, or all-cause mortality) were evaluated using competing risk analyses, with aortic valve replacement being the competing risk. Network analysis unveiled mutually exclusive communities of proteins and echocardiographic parameters, connected only through NT-proBNP (N-terminal pro-B-type natriuretic peptide). Members of the tumor necrosis factor receptor superfamily (TNFRSF1A, TNFRSF1B, and TNFRSF14), and trefoil factor-3 were major hub proteins among the circulating biomarkers. Left ventricular global longitudinal strain >-15% was associated with higher levels of proteins, primarily of inflammation and immune regulation, whereas aortic valve area <1 cm2, E/e' >15, and left atrial reservoir strain <20% were associated with higher levels of NT-proBNP. Of 14 proteins associated with the primary end point, phospholipase-C, C-X-C motif chemokine-9, and interleukin-10 receptor subunit β demonstrated the highest hazard ratios after adjusting for clinical factors (q<0.05).
Conclusions: Plasma proteins involved in inflammation and immune regulation were differentially expressed in patients with aortic stenosis with reduced left ventricular global longitudinal strain, and associated with adverse clinical outcomes. Their incorporation into aortic stenosis risk stratification warrants further assessment.
Keywords: aortic stenosis; biomarkers; inflammation; proteomics.
Figures




References
-
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, et al. 2020 ACC/AHA guideline for the Management of Patients with Valvular Heart Disease: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2021;143:e72–e227. doi: 10.1161/CIR.0000000000000923 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
