

Preclinical evaluation of targeted therapies for central nervous system metastases
- PMID: 39344915
- PMCID: PMC11463968
- DOI: 10.1242/dmm.050836
Preclinical evaluation of targeted therapies for central nervous system metastases
Abstract
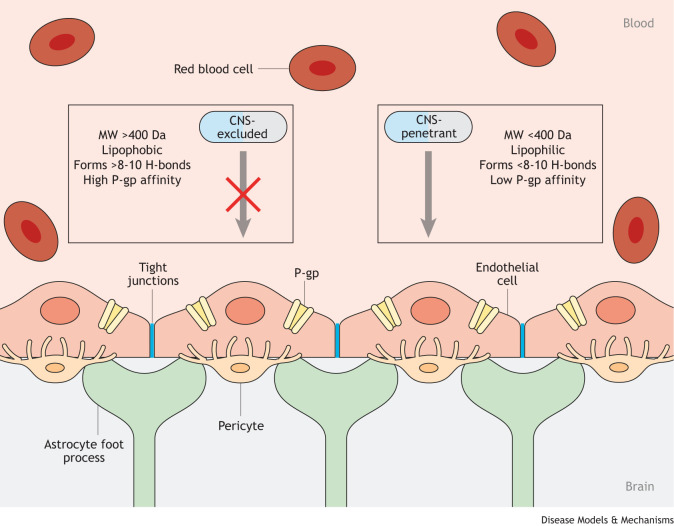
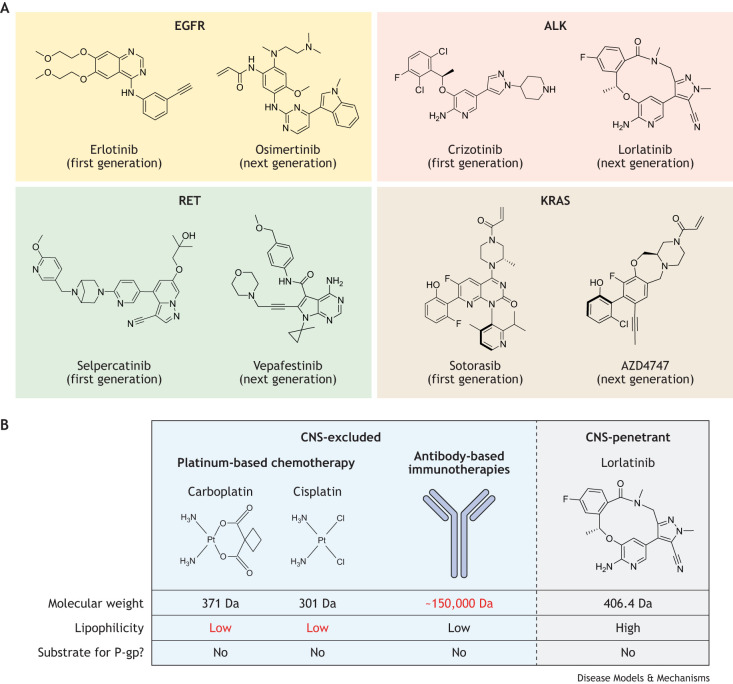
The central nervous system (CNS) represents a site of sanctuary for many metastatic tumors when systemic therapies that control the primary tumor cannot effectively penetrate intracranial lesions. Non-small cell lung cancers (NSCLCs) are the most likely of all neoplasms to metastasize to the brain, with up to 60% of patients developing CNS metastases during the disease process. Targeted therapies such as tyrosine kinase inhibitors (TKIs) have helped reduce lung cancer mortality but vary considerably in their capacity to control CNS metastases. The ability of these therapies to effectively target lesions in the CNS depends on several of their pharmacokinetic properties, including blood-brain barrier permeability, affinity for efflux transporters, and binding affinity for both plasma and brain tissue. Despite the existence of numerous preclinical models with which to characterize these properties, many targeted therapies have not been rigorously tested for CNS penetration during the discovery process, whereas some made it through preclinical testing despite poor brain penetration kinetics. Several TKIs have now been engineered with the characteristics of CNS-penetrant drugs, with clinical trials proving these efforts fruitful. This Review outlines the extent and variability of preclinical evidence for the efficacy of NSCLC-targeted therapies, which have been approved by the US Food and Drug Administration (FDA) or are in development, for treating CNS metastases, and how these data correlate with clinical outcomes.
Keywords: Blood–brain barrier; Central nervous system metastasis; Non-small cell lung cancer; Targeted therapy.
© 2024. Published by The Company of Biologists Ltd.
Conflict of interest statement
Competing interests A.J.P., J.D.H., T.S.Z. and I.O. report no potential conflicts of interest. K.W. and I.M. are employees of Taiho Pharmaceutical Company. R.S. has received research grants from Helsinn Healthcare SA, Loxo Oncology, Elevation Oncology and Merus, all unrelated to the current article.
Figures
Similar articles
-
Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors for Central Nervous System Metastases from Non-Small Cell Lung Cancer.Oncologist. 2018 Oct;23(10):1199-1209. doi: 10.1634/theoncologist.2017-0572. Epub 2018 Apr 12. Oncologist. 2018. PMID: 29650684 Free PMC article. Review.
-
AZD3759, a BBB-penetrating EGFR inhibitor for the treatment of EGFR mutant NSCLC with CNS metastases.Sci Transl Med. 2016 Dec 7;8(368):368ra172. doi: 10.1126/scitranslmed.aag0976. Sci Transl Med. 2016. PMID: 27928026
-
Molecular mechanism of type ib MET inhibitors and their potential for CNS tumors.Sci Rep. 2025 Feb 26;15(1):6926. doi: 10.1038/s41598-025-85631-w. Sci Rep. 2025. PMID: 40011494 Free PMC article.
-
Pharmacokinetic considerations in the treatment of CNS tumours.Clin Pharmacokinet. 2006;45(9):871-903. doi: 10.2165/00003088-200645090-00002. Clin Pharmacokinet. 2006. PMID: 16928151 Review.
-
Deriving therapies for children with primary CNS tumors using pharmacokinetic modeling and simulation of cerebral microdialysis data.Eur J Pharm Sci. 2014 Jun 16;57:41-7. doi: 10.1016/j.ejps.2013.11.010. Epub 2013 Nov 20. Eur J Pharm Sci. 2014. PMID: 24269626 Free PMC article. Review.
Cited by
-
Identification of alkynyl nicotinamide HSN748 as a RET solvent-front mutant inhibitor with intracranial efficacy.RSC Med Chem. 2025 May 28. doi: 10.1039/d5md00245a. Online ahead of print. RSC Med Chem. 2025. PMID: 40496186 Free PMC article.
-
Integrative single-cell and exosomal multi-omics uncovers SCNN1A and EFNA1 as non-invasive biomarkers and drivers of ovarian cancer metastasis.Front Immunol. 2025 Jul 25;16:1630794. doi: 10.3389/fimmu.2025.1630794. eCollection 2025. Front Immunol. 2025. PMID: 40787466 Free PMC article.
References
-
- Agarwal, S., Sane, R., Gallardo, J. L., Ohlfest, J. R. and Elmquist, W. F. (2010). Distribution of gefitinib to the brain is limited by P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2)-mediated active efflux. J. Pharmacol. Exp. Ther. 334, 147-155. 10.1124/jpet.110.167601 - DOI - PMC - PubMed
-
- Ahn, M.-J., Kim, D.-W., Cho, B. C., Kim, S.-W., Lee, J. S., Ahn, J.-S., Kim, T. M., Lin, C.-C., Kim, H. R. and John, T. (2017). Activity and safety of AZD3759 in EGFR-mutant non-small-cell lung cancer with CNS metastases (BLOOM): a phase 1, open-label, dose-escalation and dose-expansion study. Lancet Respir. Med. 5, 891-902. 10.1016/S2213-2600(17)30378-8 - DOI - PubMed
-
- Aizer, A. A., Lamba, N., Ahluwalia, M. S., Aldape, K., Boire, A., Brastianos, P. K., Brown, P. D., Camidge, D. R., Chiang, V. L., Davies, M. A.et al. (2022). Brain metastases: A Society for Neuro-Oncology (SNO) consensus review on current management and future directions. Neuro Oncol. 24, 1613-1646. 10.1093/neuonc/noac118 - DOI - PMC - PubMed
-
- Antoniou, D., Kyprianou, K., Stathopoulos, G. P., Skarleas, C., Kolitsi, G., Veslemes, M., Dimitroulis, J., Giamboudakis, P., Marosis, K. and Armenaki, O. (2005). Response to radiotherapy in brain metastases and survival of patients with non-small cell lung cancer. Oncol. Rep. 14, 733-736. 10.3892/or.14.3.733 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
