

Prevalence of the cefazolin inoculum effect (CzIE) in nasal colonizing methicillin-susceptible Staphylococcus aureus in patients from intensive care units in Colombia and use of a modified rapid nitrocefin test for detection
- PMID: 39345182
- PMCID: PMC11539226
- DOI: 10.1128/aac.00898-24
Prevalence of the cefazolin inoculum effect (CzIE) in nasal colonizing methicillin-susceptible Staphylococcus aureus in patients from intensive care units in Colombia and use of a modified rapid nitrocefin test for detection
Abstract
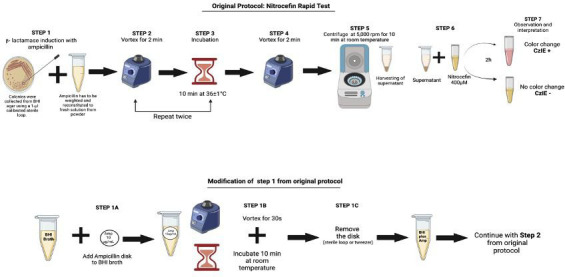
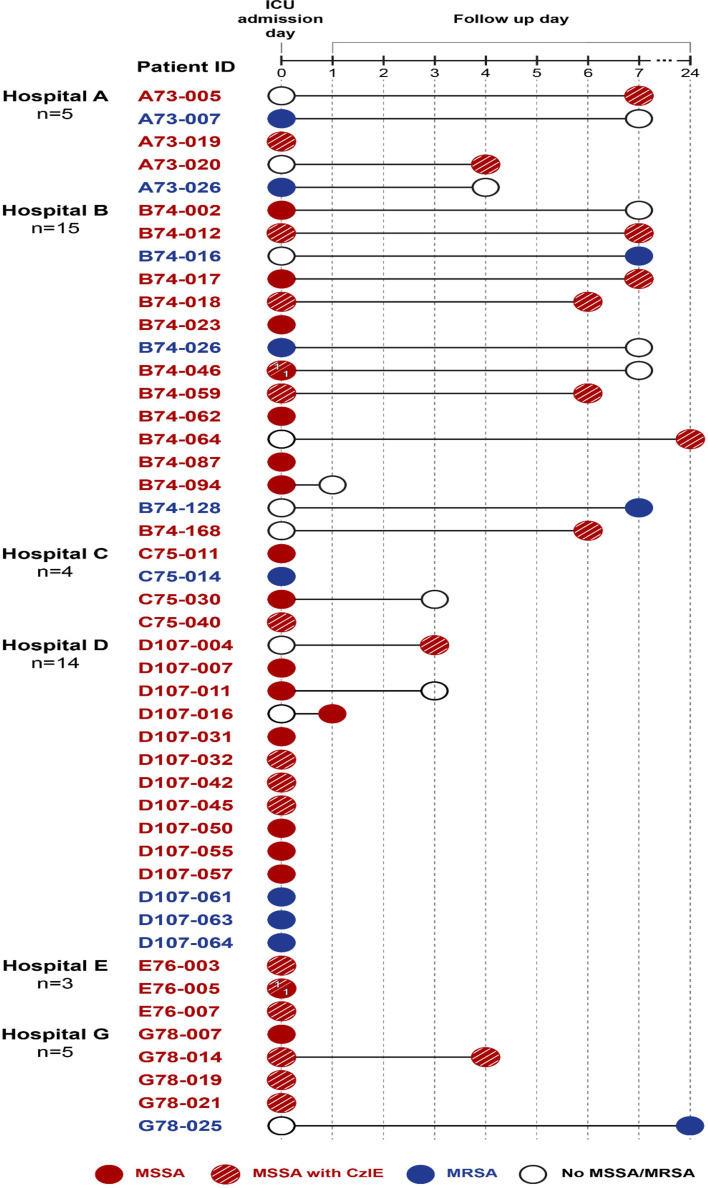
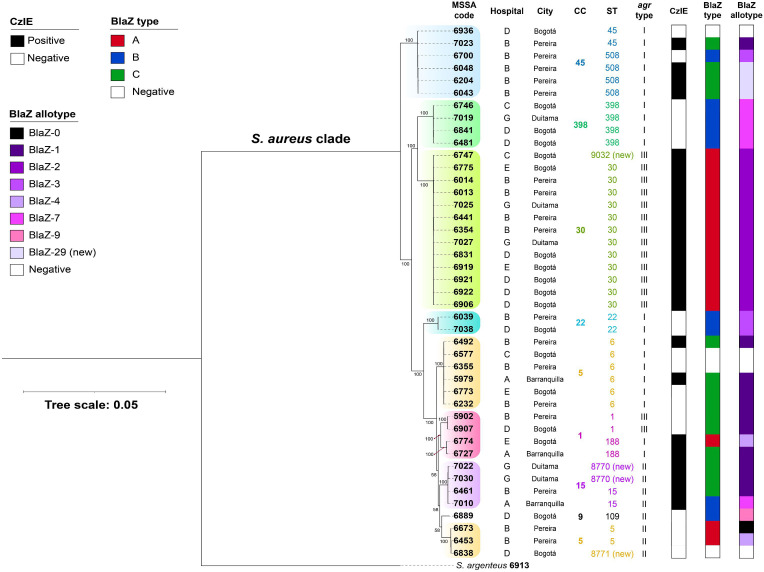
The cefazolin inoculum effect (CzIE) has been associated with poor clinical outcomes in patients with methicillin-susceptible Staphylococcus aureus (MSSA) infections. We aimed to investigate the point prevalence of the CzIE among nasal colonizing MSSA isolates from ICU patients in a multicenter study in Colombia (2019-2023). Patients underwent nasal swabs to assess for S. aureus colonization on admission to the ICU, and some individuals had follow-up swabs. We performed cefazolin MIC by broth microdilution using standard and high inoculum and developed a modified nitrocefin-based rapid test to detect the CzIE. Whole-genome sequencing was carried out to characterize BlaZ types and allotypes, phylogenomics, and Agr-typing. A total of 352 patients were included; 46/352 (13%) patients were colonized with S. aureus and 22% (10/46) and 78% (36/46) with MRSA and MSSA, respectively. Among 36 patients who contributed with 43 MSSA colonizing isolates, 21/36 (58%) had MSSA exhibiting the CzIE. BlaZ type A and BlaZ-2 were the predominant type and allotype in 56% and 52%, respectively. MSSA belonging to CC30 were highly associated with the CzIE, and single-nucleotide polymorphism (SNP) analyses supported possible transmission of MSSA exhibiting the CzIE among some patients of the same unit. The modified nitrocefin rapid test had 100%, 94.4%, and 97.7% sensitivity, specificity, and accuracy, respectively. We found a high point prevalence of the CzIE in MSSA colonizing the nares of critically ill patients in Colombia. A modified rapid test was highly accurate in detecting the CzIE in this patient population.
Keywords: Colombia; MSSA; cefazolin; inoculum effect; intensive care unit.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Update of
-
Prevalence of the Cefazolin Inoculum Effect (CzIE) in Nasal Colonizing Methicillin-Susceptible Staphylococcus aureus in Patients from Intensive Care Units in Colombia and Use of a Modified Rapid Nitrocefin Test for Detection.medRxiv [Preprint]. 2024 Jul 11:2024.07.11.24309236. doi: 10.1101/2024.07.11.24309236. medRxiv. 2024. Update in: Antimicrob Agents Chemother. 2024 Nov 6;68(11):e0089824. doi: 10.1128/aac.00898-24. PMID: 39040169 Free PMC article. Updated. Preprint.
Similar articles
-
Prevalence of the Cefazolin Inoculum Effect (CzIE) in Nasal Colonizing Methicillin-Susceptible Staphylococcus aureus in Patients from Intensive Care Units in Colombia and Use of a Modified Rapid Nitrocefin Test for Detection.medRxiv [Preprint]. 2024 Jul 11:2024.07.11.24309236. doi: 10.1101/2024.07.11.24309236. medRxiv. 2024. Update in: Antimicrob Agents Chemother. 2024 Nov 6;68(11):e0089824. doi: 10.1128/aac.00898-24. PMID: 39040169 Free PMC article. Updated. Preprint.
-
Novel Insights into the Classification of Staphylococcal β-Lactamases in Relation to the Cefazolin Inoculum Effect.Antimicrob Agents Chemother. 2020 Apr 21;64(5):e02511-19. doi: 10.1128/AAC.02511-19. Print 2020 Apr 21. Antimicrob Agents Chemother. 2020. PMID: 32071048 Free PMC article.
-
A Test for the Rapid Detection of the Cefazolin Inoculum Effect in Methicillin-Susceptible Staphylococcus aureus.J Clin Microbiol. 2021 Mar 19;59(4):e01938-20. doi: 10.1128/JCM.01938-20. Print 2021 Mar 19. J Clin Microbiol. 2021. PMID: 33536292 Free PMC article.
-
Antibiotic Resistance in the Treatment of Staphylococcus aureus Keratitis: a 20-Year Review.Cornea. 2015 Jun;34(6):698-703. doi: 10.1097/ICO.0000000000000431. Cornea. 2015. PMID: 25811722 Free PMC article. Review.
-
Clinical significance of cefazolin inoculum effect in serious MSSA infections: a systematic review.JAC Antimicrob Resist. 2024 May 6;6(3):dlae069. doi: 10.1093/jacamr/dlae069. eCollection 2024 Jun. JAC Antimicrob Resist. 2024. PMID: 38716403 Free PMC article. Review.
Cited by
-
Optimizing cefazolin dosing for central nervous system infections: insights from population pharmacokinetics and Monte Carlo simulations.Antimicrob Agents Chemother. 2025 Jul 2;69(7):e0185724. doi: 10.1128/aac.01857-24. Epub 2025 May 20. Antimicrob Agents Chemother. 2025. PMID: 40391958 Free PMC article.
-
Validation of a modified rapid test to detect the cefazolin inoculum effect in methicillin-susceptible Staphylococcus aureus from bloodstream infections in hospitals from North and Latin America.J Antimicrob Chemother. 2025 May 2;80(5):1437-1444. doi: 10.1093/jac/dkaf093. J Antimicrob Chemother. 2025. PMID: 40126549
References
-
- Fraser TG, Fatica C, Scarpelli M, Arroliga AC, Guzman J, Shrestha NK, Hixson E, Rosenblatt M, Gordon SM, Procop GW. 2010. Decrease in Staphylococcus aureus colonization and hospital-acquired infection in a medical intensive care unit after institution of an active surveillance and decolonization program. Infect Control Hosp Epidemiol 31:779–783. doi:10.1086/654001 - DOI - PubMed
-
- Wertheim HFL, Vos MC, Ott A, van Belkum A, Voss A, Kluytmans J, van Keulen PHJ, Vandenbroucke-Grauls C, Meester MHM, Verbrugh HA. 2004. Risk and outcome of nosocomial Staphylococcus aureus bacteraemia in nasal carriers versus non-carriers. Lancet 364:703–705. doi:10.1016/S0140-6736(04)16897-9 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P01 AI152999/AI/NIAID NIH HHS/United States
- 130880764152-CT 776-2018/Ministerio de Ciencia, Tecnología e Innovación (Minciencias)
- R01 AI134637/AI/NIAID NIH HHS/United States
- PCI 2023-002/Universidad El Bosque (UEB)
- T32AI179595/HHS | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- K24AI121296/HHS | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- R01AI173138/HHS | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- R01AI134637/HHS | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- R01 AI173138/AI/NIAID NIH HHS/United States
- P01AI152999/HHS | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- R01AI148342/HHS | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- K24 AI121296/AI/NIAID NIH HHS/United States
- T32 AI179595/AI/NIAID NIH HHS/United States
- R01 AI148342/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
