

Transurethral resection and other minimally invasive treatment options for BPH: would we treat ourselves as we treat our patients? Results from EAU Section of Uro-Technology (ESUT) decision-making survey among urologists
- PMID: 39345310
- PMCID: PMC11428359
- DOI: 10.5173/ceju.2023.278
Transurethral resection and other minimally invasive treatment options for BPH: would we treat ourselves as we treat our patients? Results from EAU Section of Uro-Technology (ESUT) decision-making survey among urologists
Abstract
Introduction: With the introduction of novel treatment options for benign prostatic hyperplasia (BPH), decision making regarding surgical management has become ever more complex. Factors such as clinical exposure, equipment availability, patient characteristics and hospital setting may affect what treatment is offered and an informed patient choice. The aim of this study was to investigate how urologists help patients make decisions regarding BPH management and whether their practice would differ if they were the patient themselves.
Material and methods: A 52-question survey presenting hypothetical clinical scenarios was distributed to European urologists and trainees/residents online and in person. In each scenario, regarding treatment options for BPH, the participant considered themselves firstly as the treating clinician and secondly as the patient themselves. Details regarding the participants' clinical experience, awareness of treatment options and exposure to these options were obtained.
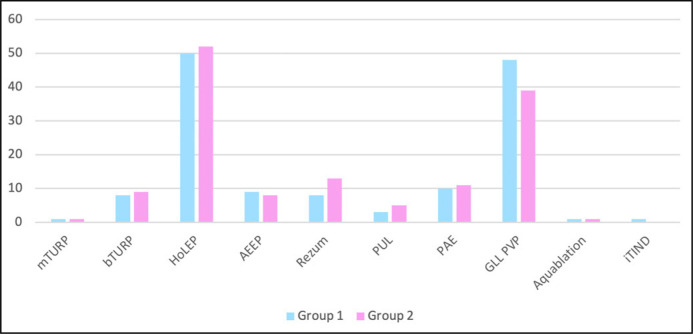
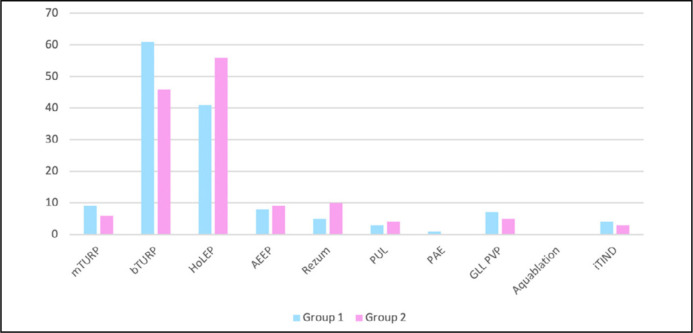
Results: There were 139 participants; 69.8% of whom were consultants, with 82.1% of participants having practiced urology for more than 5 years. A total of 59.7% of urologists consider themselves BPH specialists. Furthermore, 93.5% of those surveyed had performed transurethral resection of the prostate (TURP), whilst procedures performed the least by participants were minimally invasive surgical therapy (MIST) options. Only 17.3% had seen and 1.4% had performed all of the treatment options. When considering themselves as a patient within standard practice, there was a preference for HoLEP amongst participants.
Conclusions: The majority of urologists surveyed had minimal experience to newer BPH techniques and MIST, suggesting that more exposure is required. A higher rate of HoLEP was chosen as a treatment option for urologists themselves as a patient than what they would choose as an option for their patients.
Keywords: TURP; benign prostatic hyperplasia; laser; lower urinary tract symptoms; rezum; urolift.
Copyright by Polish Urological Association.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







Similar articles
-
Present practice and development of minimally invasive techniques, imaging and training in European urology: results of a survey of the European Society of Uro-Technology (ESUT).Eur Urol. 2003 Sep;44(3):346-51. doi: 10.1016/s0302-2838(03)00295-1. Eur Urol. 2003. PMID: 12932934
-
Energy delivery systems for treatment of benign prostatic hyperplasia: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(17):1-121. Epub 2006 Aug 1. Ont Health Technol Assess Ser. 2006. PMID: 23074487 Free PMC article.
-
Trends and attitudes in surgical management of benign prostatic hyperplasia.Can J Urol. 2012 Apr;19(2):6170-5. Can J Urol. 2012. PMID: 22512959
-
Surgical Complications in the Management of Benign Prostatic Hyperplasia Treatment.Curr Urol Rep. 2022 May;23(5):83-92. doi: 10.1007/s11934-022-01091-z. Epub 2022 Mar 9. Curr Urol Rep. 2022. PMID: 35262855 Review.
-
Complications associated with minimally invasive surgical therapies (MIST) for surgical management of benign prostatic hyperplasia: a Manufacturer and User Facility Device Experience (MAUDE) database review.World J Urol. 2023 Jul;41(7):1975-1982. doi: 10.1007/s00345-023-04440-w. Epub 2023 May 24. World J Urol. 2023. PMID: 37222779 Review.
Cited by
-
Simulation-based training in minimally invasive surgical therapies (MIST): current evidence and future directions for artificial intelligence integration-a systematic review by EAU endourology.World J Urol. 2025 Jul 18;43(1):448. doi: 10.1007/s00345-025-05834-8. World J Urol. 2025. PMID: 40681874 Free PMC article. Review.
References
-
- GBD 2019 Benign Prostatic Hyperplasia Collaborators . The global, regional, and national burden of benign prostatic hyperplasia in 204 countries and territories from 2000 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Healthy Longev. 2022; 3: e754-e776. - PMC - PubMed
-
- Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984; 132: 474-479. - PubMed
-
- Speakman M, Kirby R, Doyle S, Ioannou C. Burden of male lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) - focus on the UK. BJU Int. 2015; 115: 508-519. - PubMed
-
- Madersbacher S, Haidinger G, Temml C, Schmidbauer CP. Prevalence of lower urinary tract symptoms in Austria as assessed by an open survey of 2,096 men. Eur Urol. 1998; 34: 136-141. - PubMed
LinkOut - more resources
Full Text Sources