

This is a preprint.
Immune perturbations in human pancreas lymphatic tissues prior to and after type 1 diabetes onset
- PMID: 39345402
- PMCID: PMC11429609
- DOI: 10.1101/2024.04.23.590798
Immune perturbations in human pancreas lymphatic tissues prior to and after type 1 diabetes onset
Update in
-
Immune perturbations in human pancreas lymphatic tissues prior to and after type 1 diabetes onset.Nat Commun. 2025 May 18;16(1):4621. doi: 10.1038/s41467-025-59626-0. Nat Commun. 2025. PMID: 40383826 Free PMC article.
Abstract
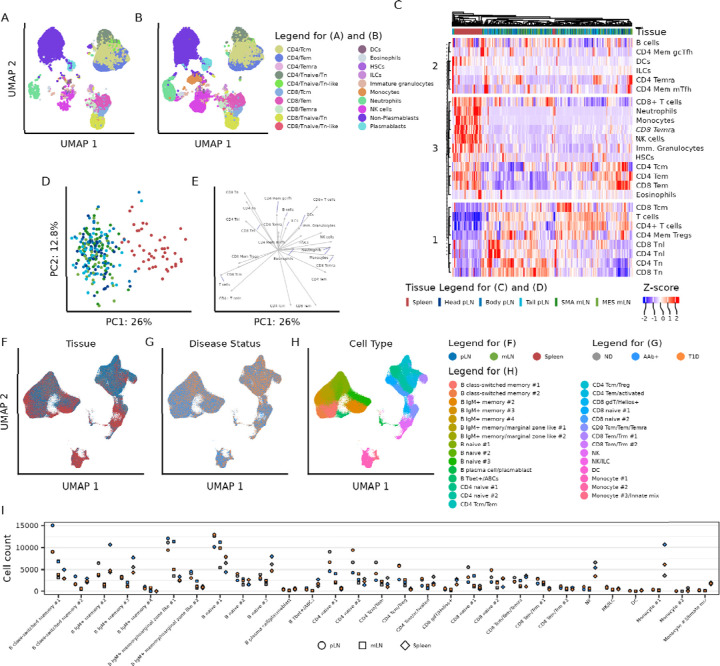
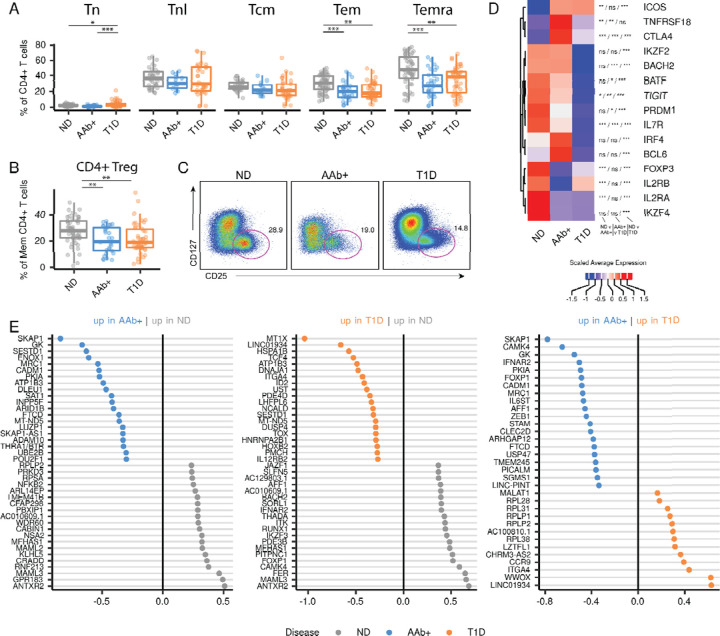
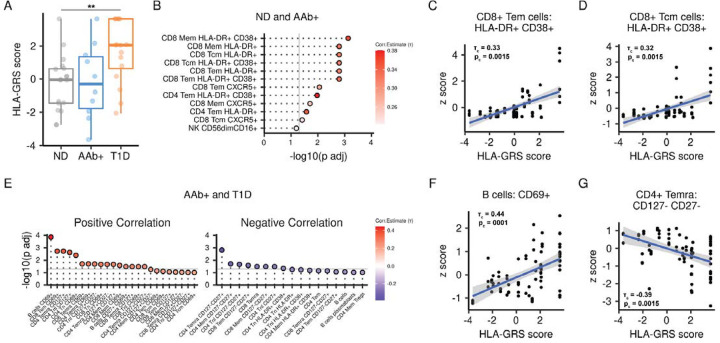
Autoimmune destruction of pancreatic β cells results in type 1 diabetes (T1D), with pancreatic immune infiltrate representing a key feature in this process. Studies of human T1D immunobiology have predominantly focused on circulating immune cells in the blood, while mouse models suggest diabetogenic lymphocytes primarily reside in pancreas-draining lymph nodes (pLN). A comprehensive study of immune cells in human T1D was conducted using pancreas draining lymphatic tissues, including pLN and mesenteric lymph nodes, and the spleen from non-diabetic control, β cell autoantibody positive non-diabetic (AAb+), and T1D organ donors using complementary approaches of high parameter flow cytometry and CITEseq. Immune perturbations suggestive of a proinflammatory environment were specific for T1D pLN and AAb+ pLN. In addition, certain immune populations correlated with high T1D genetic risk independent of disease state. These datasets form an extensive resource for profiling human lymphatic tissue immune cells in the context of autoimmunity and T1D.
Keywords: CITEseq; Type 1 diabetes; flow cytometry; mesenteric lymph node; pancreatic lymph node; spleen.
Conflict of interest statement
Ethics Declarations The authors declare no competing interests.
Figures




Similar articles
-
Immune perturbations in human pancreas lymphatic tissues prior to and after type 1 diabetes onset.Nat Commun. 2025 May 18;16(1):4621. doi: 10.1038/s41467-025-59626-0. Nat Commun. 2025. PMID: 40383826 Free PMC article.
-
Reduced Follicular Regulatory T Cells in Spleen and Pancreatic Lymph Nodes of Patients With Type 1 Diabetes.Diabetes. 2021 Dec;70(12):2892-2902. doi: 10.2337/db21-0091. Epub 2021 Oct 7. Diabetes. 2021. PMID: 34620616 Free PMC article.
-
Footprint of pancreas infiltrating and circulating immune cells throughout type 1 diabetes development.Front Endocrinol (Lausanne). 2023 Nov 10;14:1275316. doi: 10.3389/fendo.2023.1275316. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38027120 Free PMC article.
-
Pancreatic draining lymph nodes (PLNs) serve as a pathogenic hub contributing to the development of type 1 diabetes.Cell Biosci. 2023 Aug 28;13(1):156. doi: 10.1186/s13578-023-01110-7. Cell Biosci. 2023. PMID: 37641145 Free PMC article. Review.
-
Exocrine Pancreas Dysfunction in Type 1 Diabetes.Endocr Pract. 2020 Dec;26(12):1505-1513. doi: 10.4158/EP-2020-0295. Endocr Pract. 2020. PMID: 33471743 Free PMC article. Review.
References
-
- Insel R. A., Dunne J. L., Atkinson M. A., Chiang J. L., Dabelea D., Gottlieb P. A., Greenbaum C. J., Herold K. C., Krischer J. P., Lernmark Å., Ratner R. E., Rewers M. J., Schatz D. A., Skyler J. S., Sosenko J. M. & Ziegler A.-G. Staging presymptomatic type 1 diabetes: a scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care 38, 1964–1974 (2015). - PMC - PubMed
-
- Williams G. M., Long A. E., Wilson I. V., Aitken R. J., Wyatt R. C., McDonald T. J., Wong F. S., Hattersley A. T., Williams A. J. K., Bingley P. J. & Gillespie K. M. Beta cell function and ongoing autoimmunity in long-standing, childhood onset type 1 diabetes. Diabetologia 59, 2722–2726 (2016). - PMC - PubMed
-
- Gubitosi-Klug R. A., Braffett B. H., Hitt S., Arends V., Uschner D., Jones K., Diminick L., Karger A. B., Paterson A. D., Roshandel D., Marcovina S., Lachin J. M., Steffes M., Palmer J. P. & DCCT/EDIC Research Group. Residual β cell function in long-term type 1 diabetes associates with reduced incidence of hypoglycemia. J. Clin. Invest. 131, (2021). - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources