

This is a preprint.
Contributions of mechanical loading and hormonal changes to eccentric hypertrophy during volume overload: a Bayesian analysis using logic-based network models
- PMID: 39345523
- PMCID: PMC11429691
- DOI: 10.1101/2024.09.12.612768
Contributions of mechanical loading and hormonal changes to eccentric hypertrophy during volume overload: a Bayesian analysis using logic-based network models
Update in
-
Contributions of mechanical loading and hormonal changes to eccentric hypertrophy during volume overload: A Bayesian analysis using logic-based network models.PLoS Comput Biol. 2025 Apr 16;21(4):e1012390. doi: 10.1371/journal.pcbi.1012390. eCollection 2025 Apr. PLoS Comput Biol. 2025. PMID: 40238825 Free PMC article.
Abstract
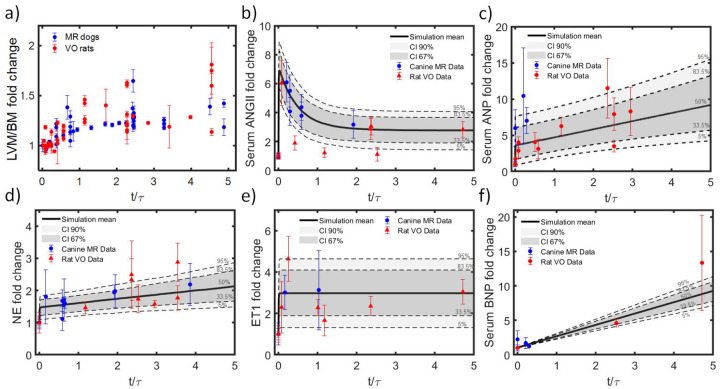
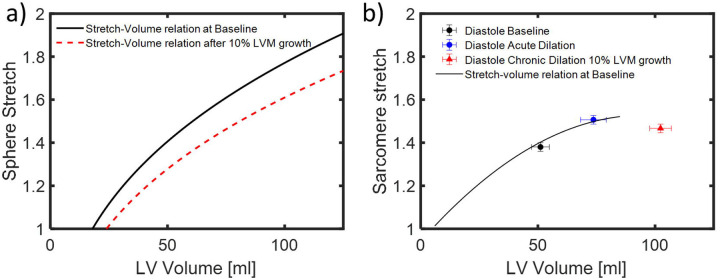
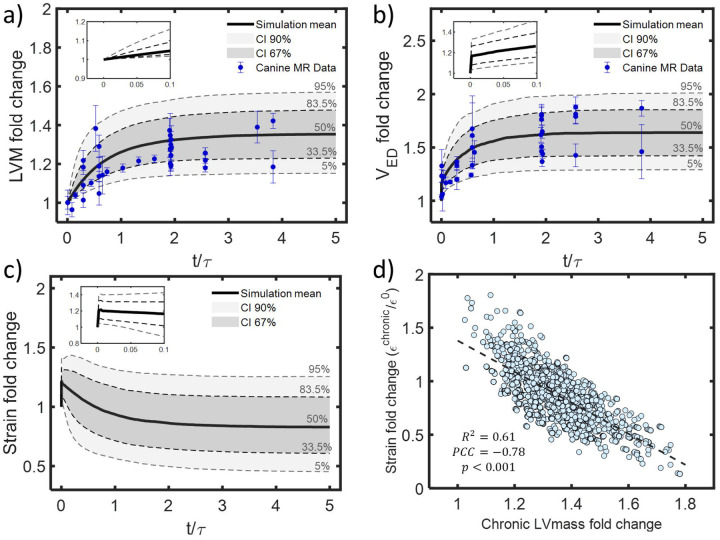
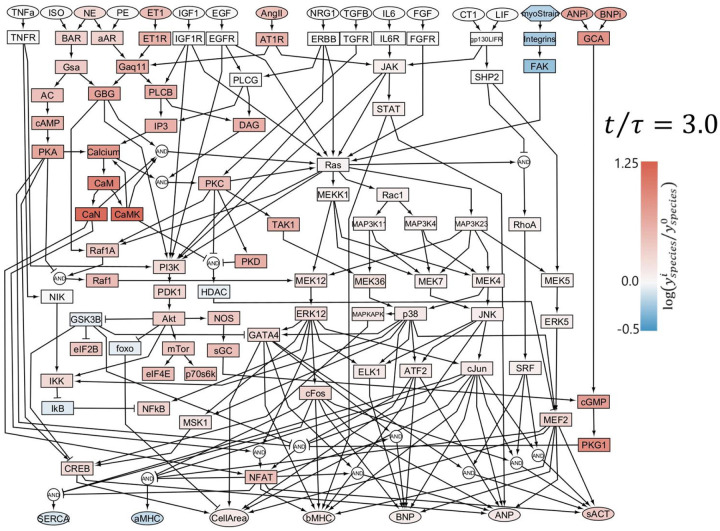
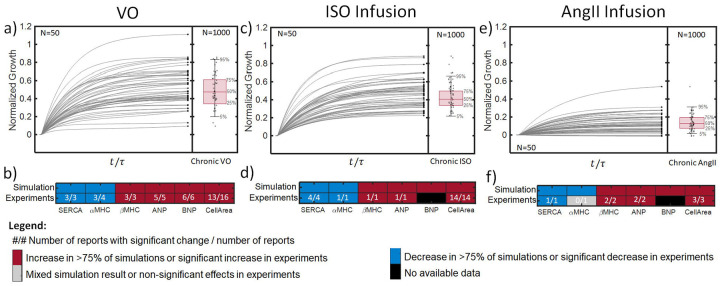
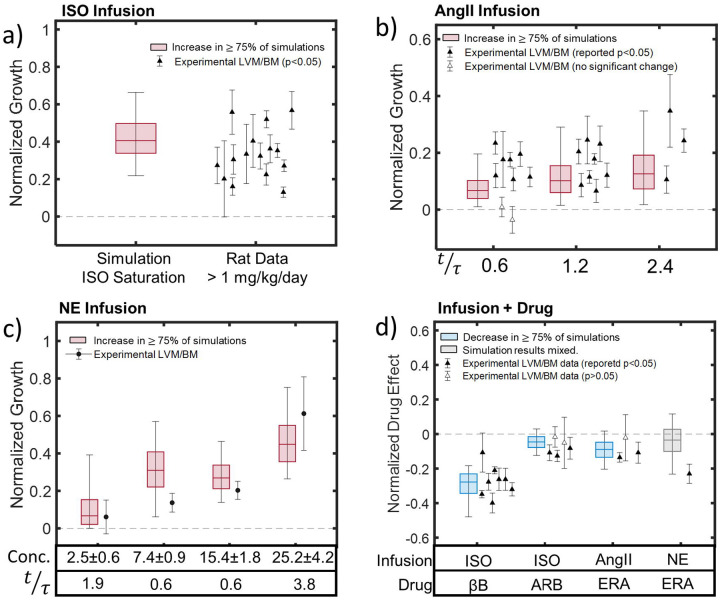
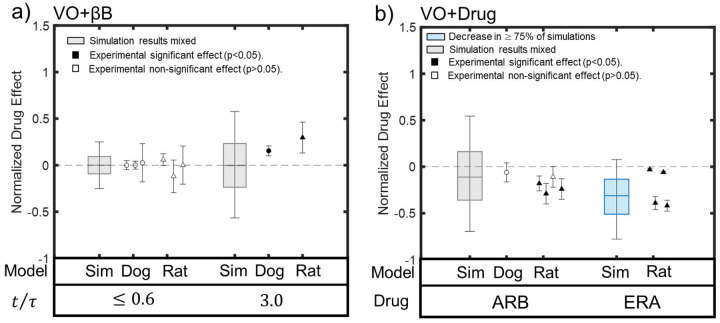
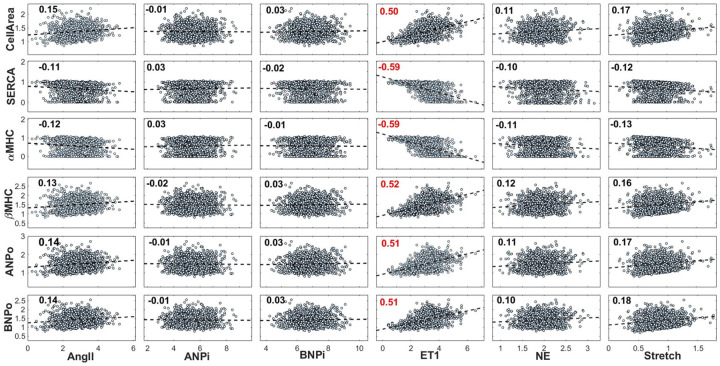
Primary mitral regurgitation (MR) is a pathology that alters mechanical loading on the left ventricle, triggers an array of compensatory neurohormonal responses, and induces a distinctive ventricular remodeling response known as eccentric hypertrophy. Drug therapies may alleviate symptoms, but only mitral valve repair or replacement can provide significant recovery of cardiac function and dimensions. Questions remain about the optimal timing of surgery, with 20% of patients developing systolic dysfunction post-operatively despite being treated according to the current guidelines. Thus, better understanding of the hypertrophic process in the setting of ventricular volume overload (VO) is needed to improve and better personalize the management of MR. To address this knowledge gap, we employ a Bayesian approach to combine data from 70 studies on experimental volume overload in dogs and rats and use it to calibrate a logic-based network model of hypertrophic signaling in myocytes. The calibrated model predicts that growth in experimental VO is mostly driven by the neurohormonal response, with an initial increase in myocardial tissue stretch being compensated by subsequent remodeling fairly early in the time course of VO. This observation contrasts with a common perception that volume-overload hypertrophy is driven primarily by increased myocyte strain. The model reproduces many aspects of 43 studies not used in its calibration, including infusion of individual hypertrophic agonists alone or in combination with various drugs commonly employed to treat heart failure, as well as administration of some of those drugs in the setting of experimental volume overload. We believe this represents a promising approach to using the known structure of an intracellular signaling network to integrate information from multiple studies into quantitative predictions of the range of expected responses to potential interventions in the complex setting of cardiac hypertrophy driven by a combination of hormonal and mechanical factors.
Conflict of interest statement
Competing interest: The authors have no competing interests to declare that are relevant to the content of this article.
Figures
Similar articles
-
Contributions of mechanical loading and hormonal changes to eccentric hypertrophy during volume overload: A Bayesian analysis using logic-based network models.PLoS Comput Biol. 2025 Apr 16;21(4):e1012390. doi: 10.1371/journal.pcbi.1012390. eCollection 2025 Apr. PLoS Comput Biol. 2025. PMID: 40238825 Free PMC article.
-
An updated Lagrangian constrained mixture model of pathological cardiac growth and remodelling.Acta Biomater. 2023 Aug;166:375-399. doi: 10.1016/j.actbio.2023.05.022. Epub 2023 May 16. Acta Biomater. 2023. PMID: 37201740
-
A single strain-based growth law predicts concentric and eccentric cardiac growth during pressure and volume overload.Mech Res Commun. 2012 Jun 1;42:40-50. doi: 10.1016/j.mechrescom.2011.11.004. Epub 2011 Nov 22. Mech Res Commun. 2012. PMID: 22639476 Free PMC article.
-
[Is secondary myocardial hypertrophy a physiological or pathological adaptive mechanism?].Z Kardiol. 1982 Aug;71(8):489-96. Z Kardiol. 1982. PMID: 6215776 Review. German.
-
The relationship of left ventricular geometry and hypertrophy to left ventricular function in valvular heart disease.J Heart Valve Dis. 1995 Oct;4 Suppl 2:S132-8; discussion S138-9. J Heart Valve Dis. 1995. PMID: 8563989 Review.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous