

Impact of Frailty and Delirium Among Older Adults Admitted With Acute Decompensated Heart Failure
- PMID: 39345900
- PMCID: PMC11437933
- DOI: 10.1016/j.jacadv.2024.101274
Impact of Frailty and Delirium Among Older Adults Admitted With Acute Decompensated Heart Failure
Abstract
Background: The presence of frailty or delirium among patients hospitalized for acute decompensated heart failure (ADHF) is associated with increased mortality and prolonged hospital stay.
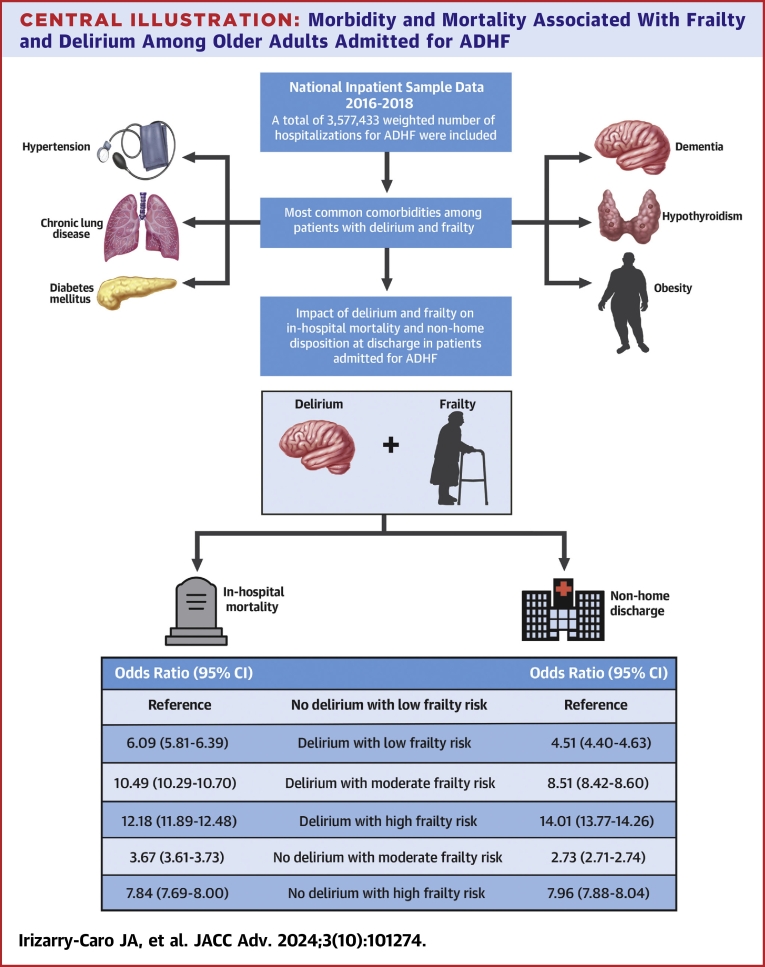
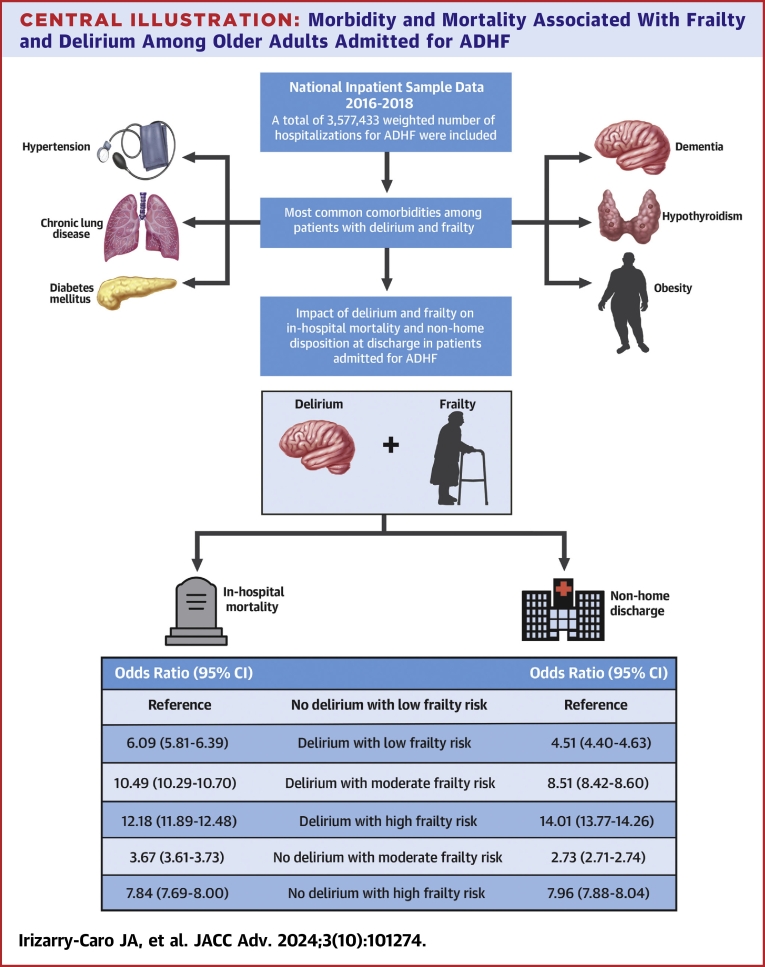
Objectives: The purpose of this study was to assess the combined effect of frailty and delirium on in-hospital mortality and disposition at discharge among older adults hospitalized with ADHF.
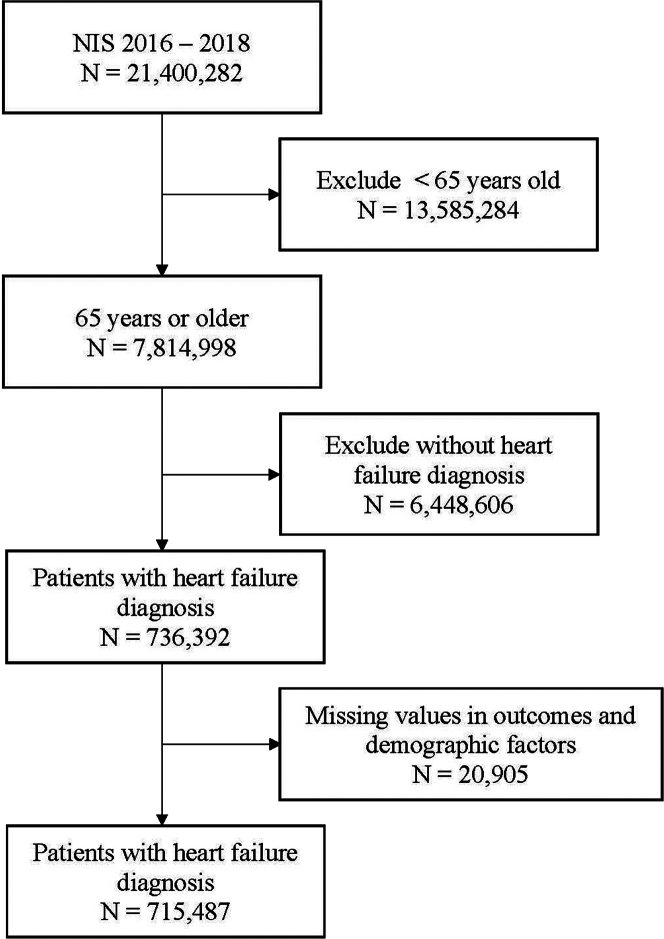
Methods: We conducted a retrospective observational study using Nationwide Inpatient Sample data from the Agency for Healthcare Research and Quality from 2016 to 2018. Patients aged 65 years or older with a diagnosis of ADHF (both with preserved and reduced left ventricular ejection fraction) were included. For analysis, we conducted a multivariable logistic regression analysis to determine OR for in-hospital mortality or nonhome discharge from delirium and frailty.
Results: A total of 3,577,433 weighted number of hospitalizations with ADHF were included. Delirium, moderate frailty risk, and high frailty risk increased the OR for in-hospital mortality (3.74; 95% CI: 3.70-3.78, 4.02; 95% CI: 3.96-4.09, and 8.63; 95% CI: 8.47-8.78, respectively) and nonhome discharge (4.21; 95% CI: 4.18-4.25, 2.95; 95% CI: 2.94-2.97, and 8.86; 95% CI: 8.78-8.94, respectively). When the combination of delirium and frailty was assessed, compared to those without delirium and with low frailty risk, the OR of mortality among those with delirium and high frailty risk was the highest at 12.18 (95% CI: 11.89-12.48). For nonhome discharge, the OR was the highest among those with delirium and high frailty risk at 14.01 (95% CI: 13.77-14.26).
Conclusions: Frailty and delirium, independently and in combination, led to higher odds of in-hospital mortality and nonhome disposition at discharge among patients hospitalized with ADHF.
Keywords: acute decompensated heart failure; delirium; disposition at discharge; frailty; mortality; older adults.
© 2024 The Authors.
Conflict of interest statement
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
Usefulness of acute delirium as a predictor of adverse outcomes in patients >65 years of age with acute decompensated heart failure.Am J Cardiol. 2011 Aug 1;108(3):402-8. doi: 10.1016/j.amjcard.2011.03.059. Am J Cardiol. 2011. PMID: 21757045
-
Delirium Among Hospitalized Older Adults With Acute Heart Failure Exacerbation.J Card Fail. 2021 Apr;27(4):453-459. doi: 10.1016/j.cardfail.2020.12.007. Epub 2021 Jan 9. J Card Fail. 2021. PMID: 33347994
-
Delirium is associated with high mortality in older adult patients with acute decompensated heart failure.BMC Geriatr. 2020 Dec 3;20(1):524. doi: 10.1186/s12877-020-01928-7. BMC Geriatr. 2020. PMID: 33272204 Free PMC article.
-
The Acute Decompensated Heart Failure National Registry (ADHERE): opportunities to improve care of patients hospitalized with acute decompensated heart failure.Rev Cardiovasc Med. 2003;4 Suppl 7:S21-30. Rev Cardiovasc Med. 2003. PMID: 14668697 Review.
-
Frailty and delirium in hospitalized older adults: A systematic review with meta-analysis.Rev Lat Am Enfermagem. 2022 Oct 17;30:e3687. doi: 10.1590/1518-8345.6120.3687. eCollection 2022. Rev Lat Am Enfermagem. 2022. PMID: 36287400 Free PMC article.
References
LinkOut - more resources
Full Text Sources
