

Imaging and Surgical Procedures After Surface-Related Collegiate Football Injuries on Artificial Turf Versus Natural Grass: Prevalence and Trends Over 15 Seasons
- PMID: 39345932
- PMCID: PMC11428175
- DOI: 10.1177/23259671241274144
Imaging and Surgical Procedures After Surface-Related Collegiate Football Injuries on Artificial Turf Versus Natural Grass: Prevalence and Trends Over 15 Seasons
Abstract
Background: Few longitudinal studies exist comparing medical procedures after football injuries on artificial and natural grass surfaces.
Purpose/hypothesis: The purpose of this study was to specifically compare imaging and surgical procedures after surface-related collegiate football injuries on artificial turf versus natural grass. It was hypothesized that there would be no difference in the incidence of imaging and surgical procedures, combined medical procedures, or combined substantial and severe injuries over time between these surfaces.
Study design: Cohort study; Level of evidence, 2.
Methods: A total of 39 universities across all Football Bowl Subdivision conferences were evaluated over 15 seasons (2006-2020). Playing surfaces evaluated were either a heavyweight artificial turf infill system (≥9.0 lb infill/ft2) or natural grass. Outcomes of interest included medical procedures across injury category, primary injury type, injury location, and specific procedures. Data involved multivariate analyses of variance (MANOVA) and Wilks λ criteria using general linear model procedures and were expressed as medical procedure incidence rates (IRs) per 10-game season.
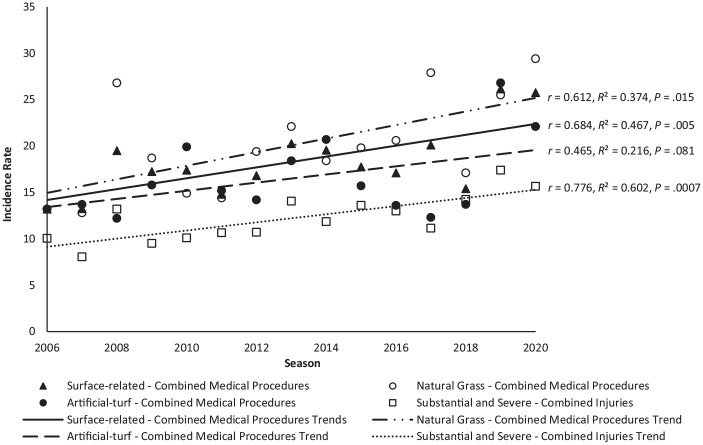
Results: Overall, 2224 games were documented: 1106 (49.7%) on artificial turf and 1118 (50.3%) on natural grass. Of the 9137 total injuries reported, 4010 (44%) were surface-related cases. MANOVA indicated significant main effects between surfaces according to imaging procedure (F 2,1738 = 4.718; P = .009), surgical procedure (F 1,539 = 5.974; P = .003), and medical diagnosis (F 2,456 = 2.643; P = .040). Post hoc analyses indicated significantly lower (P < .05) incidences on artificial turf versus natural grass, respectively, for the following outcomes: imaging procedures ordered after player-to-surface impact trauma (IR [95% CI], 1.5 [1.3-1.8] vs 2.1 [1.9-2.4]), shoe-to-surface trauma during physical contact (4.4 [4.1-4.7] vs 5.2 [4.9-5.5]), foot injuries (0.6 [0.5-0.7] vs 1.1 [0.9-1.2]), ligament sprains/tears (4.6 [4.3-4.9] vs 5.3 [5.0-5.6]), muscle strains/tears (0.2 [0.2-0.3] vs 0.7 [0.6-0.9]), surgeries performed after shoe-to-surface trauma during physical contact (1.1 [0.9-1.3] vs 1.6 [1.4-1.8]), lower body surgeries (1.8 [1.6-2.0] vs 2.3 [2.1-2.6]), and surgeries involving ligament tears (1.0 [0.9-1.2] vs 1.5 [1.3-1.7]), as well as fewer diagnoses of syndesmosis sprains/tears (0.7 [0.5-0.8] vs 1.0 [0.8-1.2]) and Lisfranc trauma (0.3 [0.2-0.4] vs 0.5 [0.4-0.7]). Trends over the 15 seasons indicated a significant rise in combined medical procedures (P = .005) and combined substantial and severe injuries (P = .0007) irrespective of surface.
Conclusion: Results indicated that collegiate football competition on heavyweight artificial turf resulted in lower incidences of imaging and surgical procedures and medical diagnoses compared with natural grass.
Keywords: MRI; radiograph; synthetic field; trauma.
© The Author(s) 2024.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from FieldTurf USA (to M.C.M.). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
Lisfranc injury: Prevalence and maintaining a high index of suspicion for optimal evaluation.Phys Sportsmed. 2022 Dec;50(6):507-514. doi: 10.1080/00913847.2021.1969218. Epub 2021 Aug 25. Phys Sportsmed. 2022. PMID: 34429021
-
Incidence, Mechanisms, and Severity of Game-Related High School Football Injuries Across Artificial Turf Systems of Various Infill Weights.Orthop J Sports Med. 2019 Mar 25;7(3):2325967119832878. doi: 10.1177/2325967119832878. eCollection 2019 Mar. Orthop J Sports Med. 2019. PMID: 30937317 Free PMC article.
-
Incidence, Mechanisms, and Severity of Match-Related Collegiate Men's Soccer Injuries on FieldTurf and Natural Grass Surfaces: A 6-Year Prospective Study.Am J Sports Med. 2017 Mar;45(3):708-718. doi: 10.1177/0363546516671715. Epub 2016 Nov 24. Am J Sports Med. 2017. PMID: 27872124
-
Lower Extremity Injury Rates on Artificial Turf Versus Natural Grass Playing Surfaces: A Systematic Review.Am J Sports Med. 2023 May;51(6):1615-1621. doi: 10.1177/03635465211069562. Epub 2022 May 20. Am J Sports Med. 2023. PMID: 35593739
-
Examining the Prevalence of Anterior Cruciate Ligament Injuries on Artificial Turf Surfaces Compared to Natural Grass Surfaces in Athletes: A Scoping Review.Cureus. 2024 Jul 3;16(7):e63770. doi: 10.7759/cureus.63770. eCollection 2024 Jul. Cureus. 2024. PMID: 39099910 Free PMC article.
References
-
- Almutawa M, Scott M, George KP, Drust B. The incidence and nature of injuries sustained on grass and 3rd generation artificial turf: a pilot study in elite Saudi National Team footballers. Phys Ther Sport. 2014;15(1):47-52. - PubMed
-
- Arden CL, Taylor NF, Feller JA, Whitehead TS, Webster KE. Sports participation 2 years after anterior cruciate ligament reconstruction in athletes who had not returned to sport at 1 year: a prospective follow-up of physical function and psychological factors in 122 athletes. Am J Sports Med. 2015;43(4):848-856. - PubMed
-
- Bahr R, Clarsen B, Ekstrand J. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br J Sports Med. 2018;52(16):1018-1021. - PubMed
-
- Balazs GC, Pavey GJ, Brelin AM, Pickett A, Keblish DJ, Rue JP. Risk of anterior cruciate ligament injury in athletes on synthetic playing surfaces: a systematic review. Am J Sports Med. 2015;43(7):1798-1804. - PubMed
LinkOut - more resources
Full Text Sources
