

Nephrotic syndrome as a possible indicator of colonic cancer: A case report
- PMID: 39345954
- PMCID: PMC11428093
- DOI: 10.3892/br.2024.1858
Nephrotic syndrome as a possible indicator of colonic cancer: A case report
Abstract
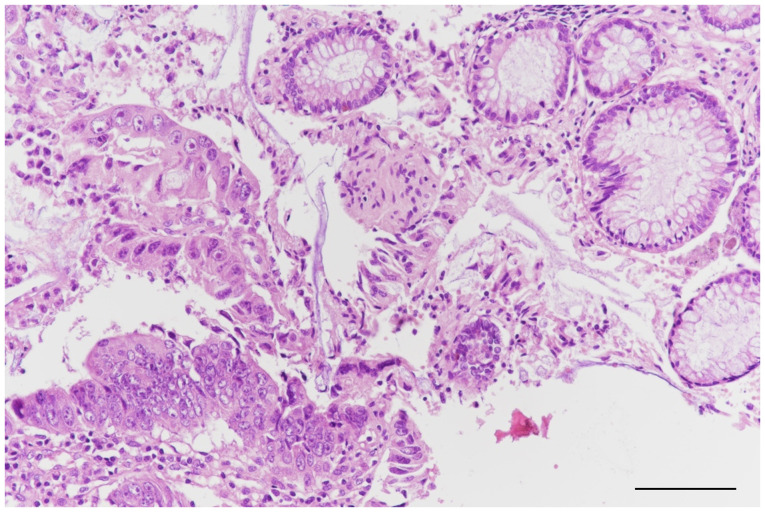
The concept of paraneoplastic syndromes encompasses a spectrum of indirect clinical manifestations caused by secretion of bioactive products by malignant cells. Paraneoplastic glomerulopathy represent a distinct clinical entity where nephrotic syndrome can arise as a manifestation of underlying malignancies, particularly solid tumors. Membranous nephropathy is notably associated with such malignancies, highlighting the intricate relationship between nephrotic syndrome and cancer. The present study reports the case of a 44-year-old Caucasian male, smoker (22 pack-years) and chronic ethanol consumer who presented in the Emergency County Hospital of Craiova in March 2018 with abdominal distension, genital and leg edema and no prior medical history. Laboratory tests revealed inflammatory syndrome (erythrocyte sedimentation rate=110 mm/h, fibrinogen, 150 mg/dl, high levels of C reactive protein=6.87 mg/dl), as well as hypoproteinemia (total protein levels=3.90 g/l), hypertriglyceridemia=213 mg/dl, hypercholesterolemia=475 mg/dl, total urinary protein excretion of 12,500 mg/24 h and normal levels of urea (38 mg/dl) and creatinine (0.90 mg/dl). After meeting the diagnostic criteria for nephrotic syndrome (edema, proteinuria, hypoalbuminemia, and hyperlipidemia, it was investigated whether the syndrome was primary or secondary in origin. Notably, an unexplained inflammatory syndrome in conjunction with elevated tumor marker levels (carbohydrate antigen 19-9, 82.47 U/ml; Carcinoembryonic antigen-CEA=9.46 ng/ml) prompted a thorough imagistic investigation, using computer tomography. A polyp was discovered during colonoscopy, prompting a biopsy. The presence of adenocarcinoma was confirmed by histopathological analysis. The only clinical manifestation of the colonic malignancy was the symptomatic presentation of nephrotic syndrome, which led to early detection of the underlying cancer. Paraneoplastic nephropathy connects kidney disease with systemic cancer, showing that renal symptoms may aid in diagnosing hidden malignancies. Nephrotic syndrome, especially membranous nephropathy, is associated with various solid tumors. The present case demonstrated that paraneoplastic syndrome, though rare, may lead to early cancer detection. Ongoing research is essential for improving understanding, targeted therapy and patient management.
Keywords: colonic cancer; nephrotic syndrome; paraneoplastic syndrome.
Copyright: © 2024 Surugiu et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






Similar articles
-
Recurrent paraneoplastic nephrotic syndrome; insights from a Lynch syndrome patient with multiple malignancies.Fam Cancer. 2024 Dec 4;24(1):11. doi: 10.1007/s10689-024-00435-7. Fam Cancer. 2024. PMID: 39630202
-
Successful treatment of renal cell carcinoma with paraneoplastic nephrotic syndrome: a case report.Front Med (Lausanne). 2025 Mar 27;12:1506592. doi: 10.3389/fmed.2025.1506592. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40212278 Free PMC article.
-
Liddle's-like syndrome associated with nephrotic syndrome secondary to membranous nephropathy: the first case report.BMC Nephrol. 2018 May 23;19(1):122. doi: 10.1186/s12882-018-0916-3. BMC Nephrol. 2018. PMID: 29792170 Free PMC article.
-
A case of paraneoplastic nephrotic syndrome in a patient with ovarian carcinoma.Yonsei Med J. 2003 Jun 30;44(3):539-43. doi: 10.3349/ymj.2003.44.3.539. Yonsei Med J. 2003. PMID: 12833596 Review.
-
Nephrotic syndrome associated with solid malignancies: a systematic review.BMC Nephrol. 2024 Jul 4;25(1):215. doi: 10.1186/s12882-024-03632-9. BMC Nephrol. 2024. PMID: 38965515 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous