

A Lifeboat for Failed Nasal Reconstructions: The Supraclavicular-Submental Sandwich Flap
- PMID: 39345999
- PMCID: PMC11436342
- DOI: 10.1055/a-2337-2131
A Lifeboat for Failed Nasal Reconstructions: The Supraclavicular-Submental Sandwich Flap
Abstract
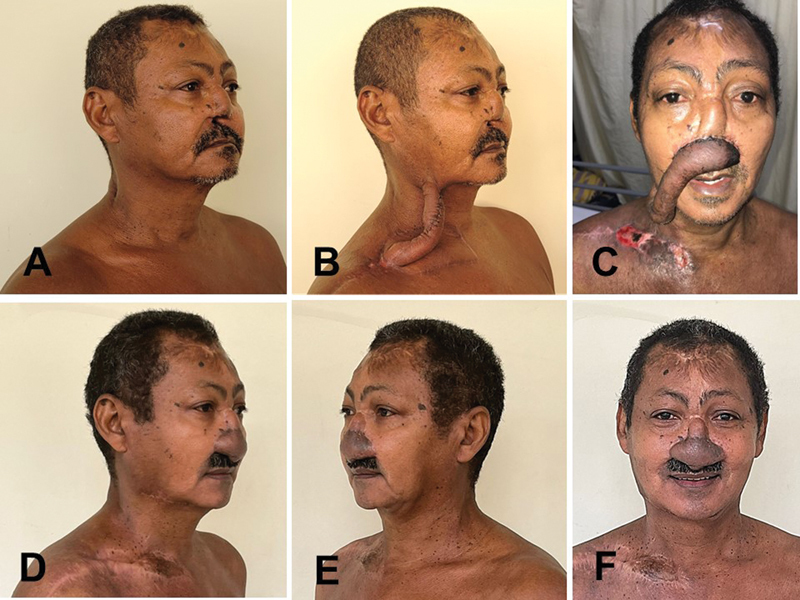
Many failures in total or subtotal nasal reconstruction result from an underestimation of the amount of skin required for an adequate result, especially for sufficient lining. Such planning errors usually lead to poor results, with exposure of structural grafts, infection, scar retraction, airway obstruction, and finally loss of projection and shape of the reconstructed nose. Reconstruction options for cases in which previous attempts have failed are always limited, as well as in cases of trauma or burns affecting the soft tissues of the forehead and face. In such complex situations, one may employ free flaps or tissue expansion, but such resources may not be always available. We describe a technique indicated for salvage surgeries in patients whose previous nasal reconstructions have failed, allowing a generous amount of tissue transfer for the nasal region. The technique combines the use of supraclavicular and submental flaps, with simple execution, not requiring microsurgical skills or devices such as tissue expanders. Done in three stages, the described technique provides enough skin for a total nasal reconstruction. The final result is obtained after subsequent refinements, and the total number of procedures is equivalent to when more sophisticated techniques are employed, such as tissue expansion or microsurgery.
Keywords: acquired; nose deformities; reconstructive surgical procedures; surgical flaps.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. ( https://creativecommons.org/licenses/by/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures




References
-
- Whitaker I S, Karoo R O, Spyrou G, Fenton O M. The birth of plastic surgery: the story of nasal reconstruction from the Edwin Smith Papyrus to the twenty-first century. Plast Reconstr Surg. 2007;120(01):327–336. - PubMed
-
- Marck K W, Palyvoda R, Bamji A, van Wingerden J J. The tubed pedicle flap centennial: its concept, origin, rise and fall. Eur J Plast Surg. 2017;40:473–478.
-
- Lamberty B GH. The supra-clavicular axial patterned flap. Br J Plast Surg. 1979;32(03):207–212. - PubMed
-
- Pallua N, Magnus Noah E.The tunneled supraclavicular island flap: an optimized technique for head and neck reconstruction Plast Reconstr Surg 200010503842–851., discussion 852–854 - PubMed
-
- Patel U A, Bayles S W, Hayden R E. The submental flap: a modified technique for resident training. Laryngoscope. 2007;117(01):186–189. - PubMed
LinkOut - more resources
Full Text Sources