

Differences in cervical sagittal parameters and muscular function among subjects with different cervical spine alignments: a surface electromyography-based cross-sectional study
- PMID: 39346046
- PMCID: PMC11438432
- DOI: 10.7717/peerj.18107
Differences in cervical sagittal parameters and muscular function among subjects with different cervical spine alignments: a surface electromyography-based cross-sectional study
Abstract
Background: We analyzed cervical sagittal parameters and muscular function in different cervical kyphosis types.
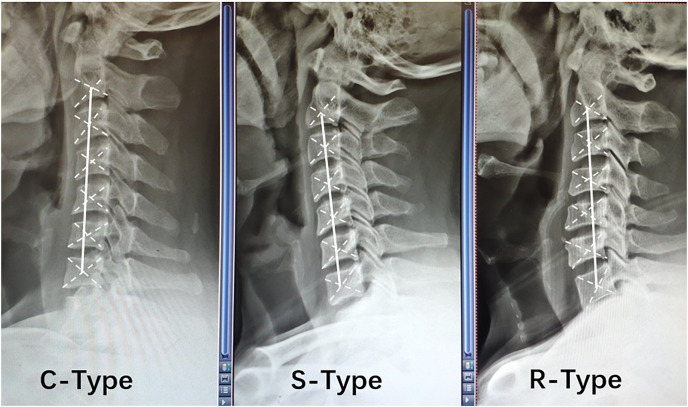
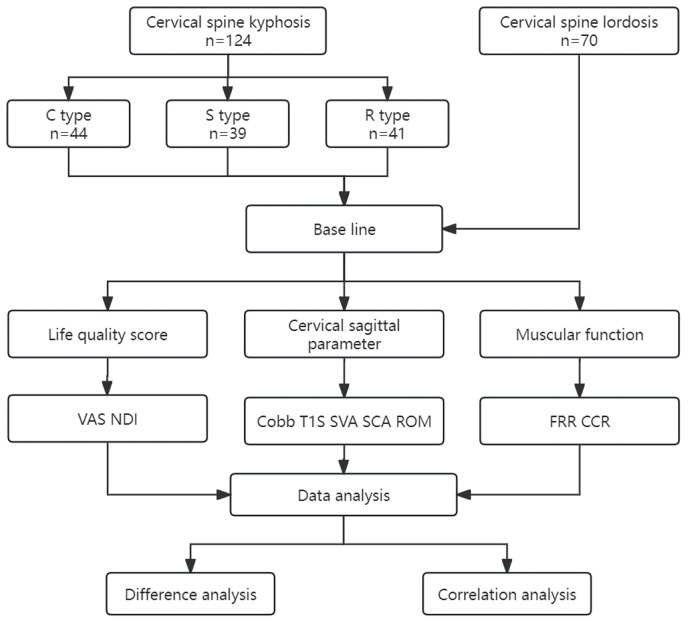
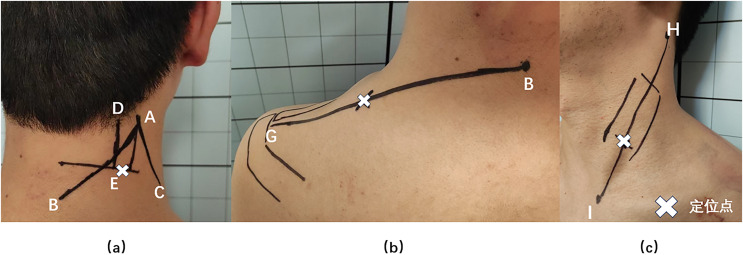
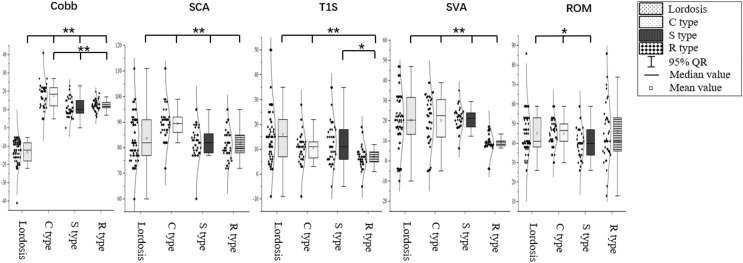
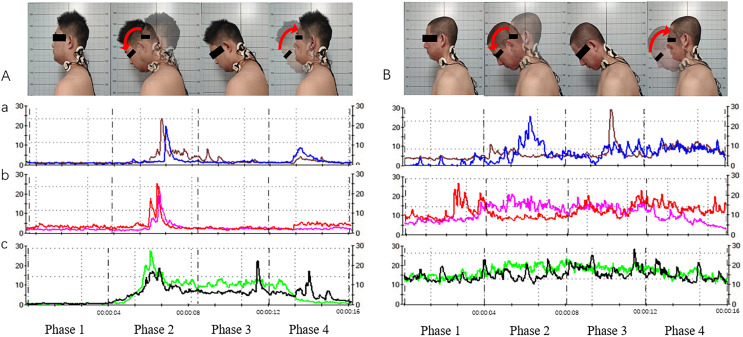
Methods: This cross-sectional study enrolled subjects with cervical spine lordosis (cervical curvature < -4°) or degenerative cervical kyphosis (cervical curvature > 4°), including C-, S-, and R-type kyphosis. We recorded patients' general information (gender, age, body mass index), visual analog scale (VAS) scores, and the Neck Disability Index (NDI). Cervical sagittal parameters including C2-C7 Cobb angle (Cobb), T1 slope (T1S), C2-C7 sagittal vertical axis (SVA), spino-cranial angle (SCA), range of motion (ROM), and muscular function (flexion-relaxation ratio (FRR) and co-contraction ratio (CCR) of neck/shoulder muscles on surface electromyography). Differences in cervical sagittal parameters and muscular function in subjects with different cervical spine alignments, and correlations between VAS scores, NDI, cervical sagittal parameters, and muscular function indices were statistically analyzed.
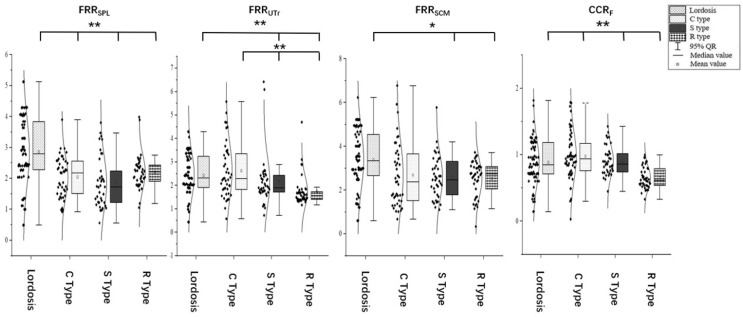
Results: The FRR of the splenius capitis (SPL), upper trapezius (UTr), and sternocleidomastoid (SCM) were higher in subjects with cervical lordosis than in subjects with cervical kyphosis. FRRSPL was higher in subjects with C-type kyphosis than in subjects with R- and S-type kyphosis (P < 0.05), and was correlated with VAS scores, Cobb angle, T1S, and SVA. FRRUTr was correlated with NDI, SCA, T1S, and SVA. FRRSCM was correlated with VAS scores and Cobb angle. CCR was correlated with SCA and SVA.
Conclusion: Cervical sagittal parameters differed among different cervical kyphosis types. FRRs and CCRs were significantly worse in R-type kyphosis than other kyphosis types. Cervical muscular functions were correlated with cervical sagittal parameters and morphological alignment.
Keywords: Cervical kyphosis; Cervical sagittal parameters; Flexion and relaxation ratio; Muscular function; Surface electromyography.
© 2024 Wang et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Brumpt E, Aubry S, Vuillier F, Tatu L. Anatomo-sonographic identification of the longissimus capitis and splenius cervicis muscles: principles for possible application to ultrasound-guided botulinum toxin injections in cervical dystonia. Surgical and Radiologic Anatomy. 2021;43(6):909–915. doi: 10.1007/s00276-020-02646-w. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
