

Rehabilitation protocols in proximal humerus fracture management: A systematic review
- PMID: 39346799
- PMCID: PMC11437559
- DOI: 10.1177/17585732231182374
Rehabilitation protocols in proximal humerus fracture management: A systematic review
Abstract
Background: Proximal humerus fractures (PHFs) are relatively common, although optimal rehabilitation is unknown. This review aims to characterize the published rehabilitation regimens utilized for PHFs.
Methods: A systematic review was performed per PRISMA guidelines, utilizing PubMed/MEDLINE, Embase, and Cochrane. All studies reporting PHF rehabilitation protocols after nonoperative management, open reduction internal fixation with a plate, or intramedullary nailing were included.
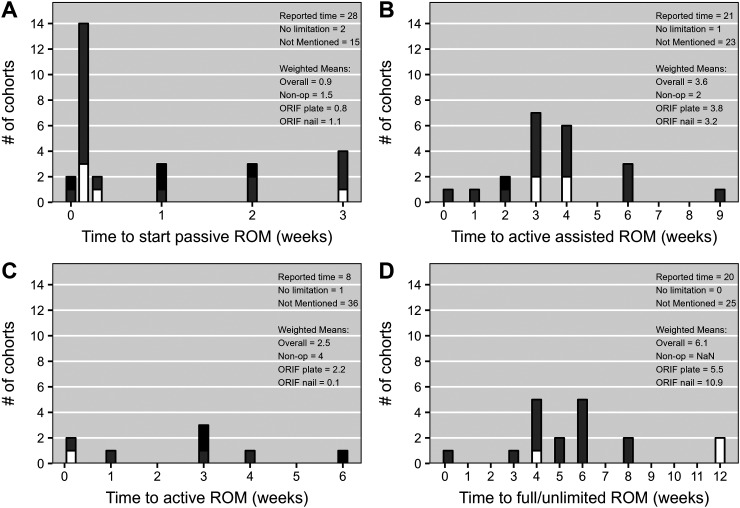
Results: Forty articles comprising 3507 patients (66% female, weighted mean age 63.5 years) were included. Substantial variability was present regardless of management. Rehabilitation modalities reported were: sling use in 34 cohorts, most commonly for three weeks; pendulum exercises in 21 cohorts, most commonly starting at post-intervention day 1; post-intervention passive range of motion (ROM) for 30 cohorts, most commonly starting at two days; active-ROM in eight cohorts, most commonly starting at three weeks; active-assisted ROM for 21 cohorts, most commonly starting at three weeks; unlimited ROM for 20 cohorts, most commonly at 4 or 6 weeks; non-weight-bearing for six cohorts, most commonly for six weeks; strengthening for 16 cohorts, most commonly at six weeks; removal of all restrictions for nine cohorts, most commonly starting at six weeks.
Conclusions: Published rehabilitation protocols for PHFs vary considerably regardless of management. Future studies comparing methods of management need to consider the influence of postoperative rehabilitation protocol heterogeneity when aggregating data from multiple sites.
Level of evidence: IV.
Keywords: Humeral; arm; conservative treatment; open reduction and internal fixation; physical therapy; shoulder; upper extremity.
© The Author(s) 2023.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.J.K is a consultant for Exactech, Inc. and LinkBio Corps not related to this study. T.W.W. receives royalties and is a consultant for Exactech, Inc. not related to this study. C.J.F is a consultant for Stryker Inc. not related to this study. K.A.H has a consultancy agreement with LinkBio Corps. The remaining authors, their immediate families, and any affiliated research foundations with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.
Figures



References
-
- Karl JW, Olson PR, Rosenwasser MP. The epidemiology of upper extremity fractures in the United States, 2009. J Orthop Trauma 2015; 29: e242‐e244. - PubMed
-
- Hao KA, Patch DA, Reed LA, et al. Factors influencing surgical management of proximal humerus fractures: do shoulder and trauma surgeons differ? J Shoulder Elbow Surg 2022; 31: e259‐e269. - PubMed
-
- Patch DA, Reed LA, Hao KA, et al. Understanding postop rehabilitation preferences in operatively managed proximal humerus fractures: do trauma and shoulder surgeons differ? J Shoulder Elbow Surg 2022; 31: 1106‐1114. - PubMed
-
- Feissli S, Audigé L, Steinitz A, et al. Treatment options for proximal humeral fractures in the older adults and their implication on personal independence. Arch Orthop Trauma Surg 2020; 140: 1971‐1976. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials