

A Systematic Review and Meta-Analysis of Synthetic Mesh Outcomes in Alloplastic Breast Reconstruction
- PMID: 39346802
- PMCID: PMC11427907
- DOI: 10.1093/asjof/ojae066
A Systematic Review and Meta-Analysis of Synthetic Mesh Outcomes in Alloplastic Breast Reconstruction
Abstract
Background: Mesh implants are frequently employed in alloplastic breast reconstruction. Notably, no mesh to date has FDA approval for this indication. Several synthetic meshes have been introduced with heterogeneous properties and outcomes.
Objectives: This study aims to systematically review synthetic mesh use in alloplastic breast reconstruction, describe rates of short-term complications, and analyze these outcomes in reports comparing synthetic and biologic meshes. The authors hypothesized data from comparative and noncomparative studies would show no significant differences between synthetic and biological meshes.
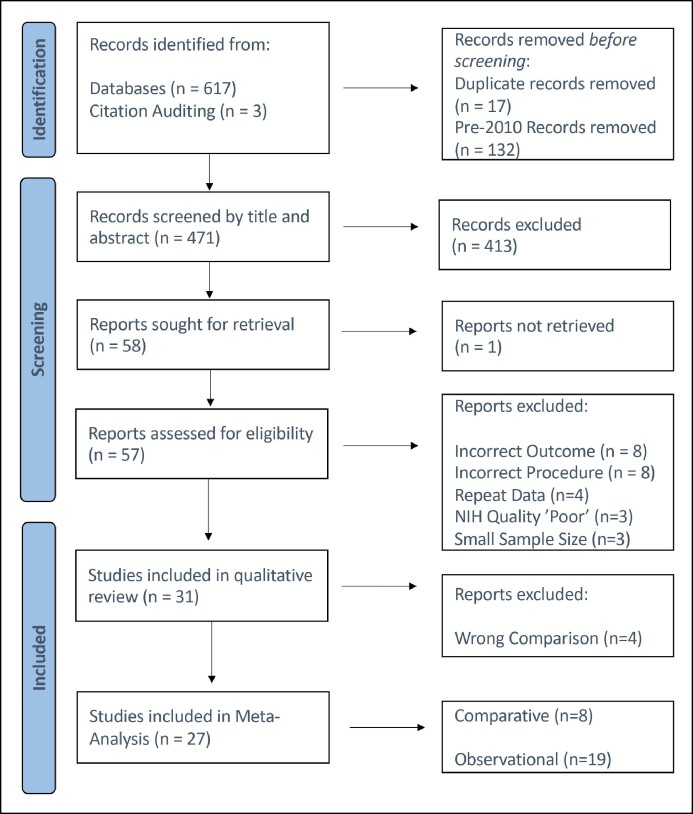
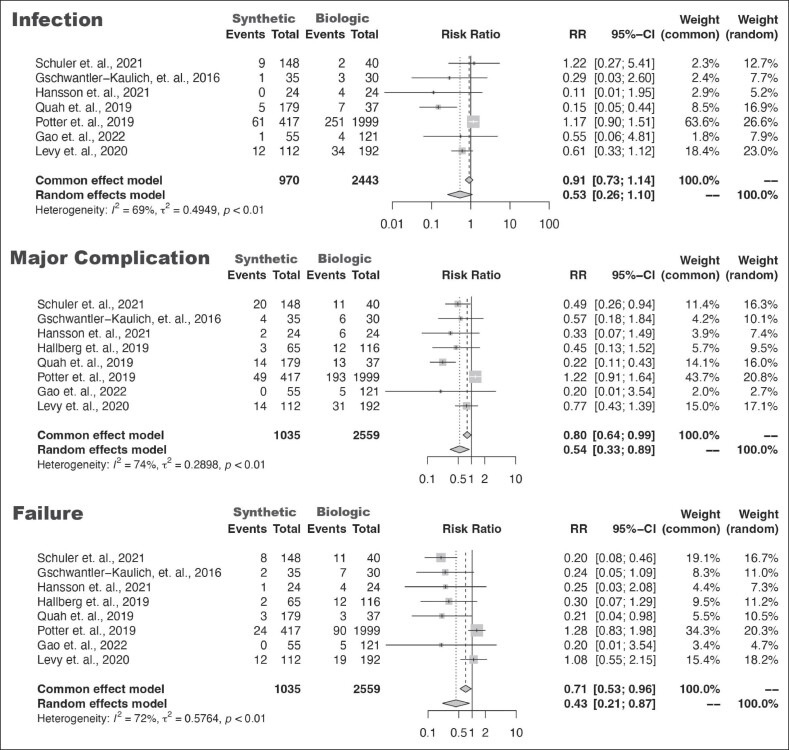
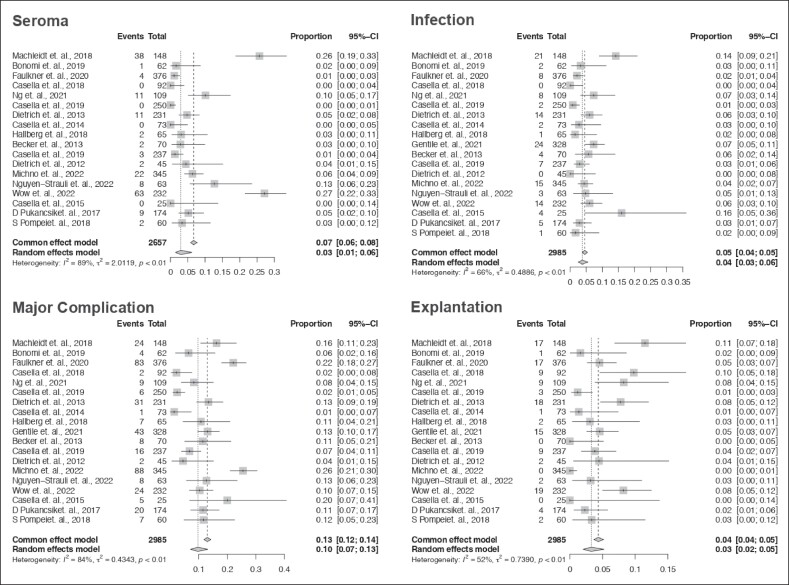
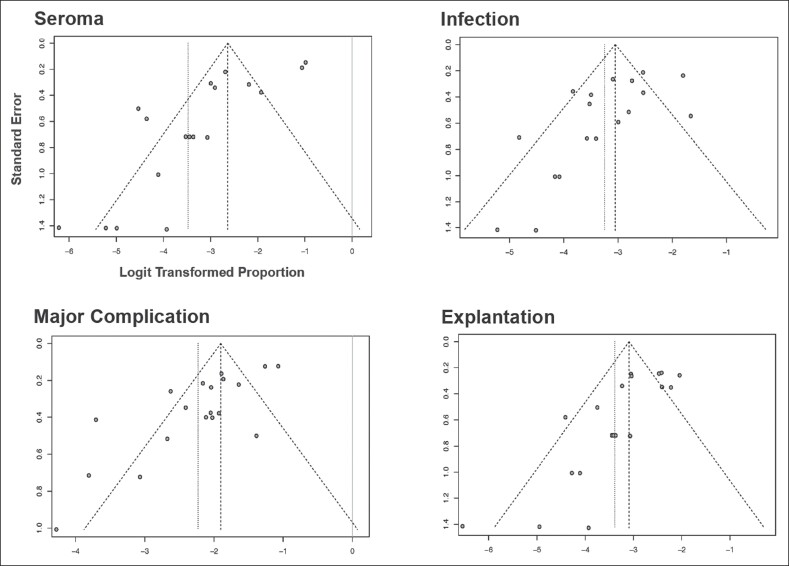
Methods: The authors conducted a systematic literature review following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Thirty-one studies reporting the use of synthetic mesh and clinical outcomes were included. Eight studies directly comparing synthetic mesh and biological mesh were meta-analyzed for relative risk (RR). Nineteen noncomparative studies were analyzed for meta-rates. Outcomes, including seroma, infection, reoperation, and explant, were assessed on a per-breast basis. Resultant models were challenged for sensitivity and bias.
Results: Meta-analysis of comparative studies demonstrated no difference in the risk of infection with synthetic mesh (RR = 0.53; 95% CI [0.26-1.10]), but a reduced risk of reoperation (RR = 0.54; 95% CI [0.33-0.89]) or explant (RR = 0.43; 95% CI [0.21-0.87]). Meta-analysis of noncomparative studies demonstrated rates of seroma = 3%; 95% CI [1%-6%], infection = 4%; 95% CI [3%-6%], reoperation = 10%; 95% CI [7%-13%], and explant = 3%; 95% CI [2%-5%]).
Conclusions: Studies comparing synthetic and biologic meshes demonstrated noninferiority of synthetic in all outcomes assessed. Noncomparative studies demonstrated rates of seroma, infection, reoperation, and explant similar to literature values for biological mesh.
Published by Oxford University Press on behalf of The Aesthetic Society 2024.
Figures
References
-
- American Society of Plastic Surgeons . 2015-2022 Plastic Surgery Statistics Report. Accessed April 4, 2024. https://www.plasticsurgery.org/news/plastic-surgery-statistics
-
- Czajka ML, Pfeifer C.. Breast cancer surgery, ed. StatPearls. StatPearls Publishing; 2022:2–12. Accessed November 22, 2022. http://www.ncbi.nlm.nih.gov/books/NBK553076/ - PubMed
Publication types
LinkOut - more resources
Full Text Sources