

Role of physiology in the management of multivessel disease among patients with acute coronary syndrome
- PMID: 39347110
- PMCID: PMC11413640
- DOI: 10.4244/AIJ-D-24-00051
Role of physiology in the management of multivessel disease among patients with acute coronary syndrome
Abstract
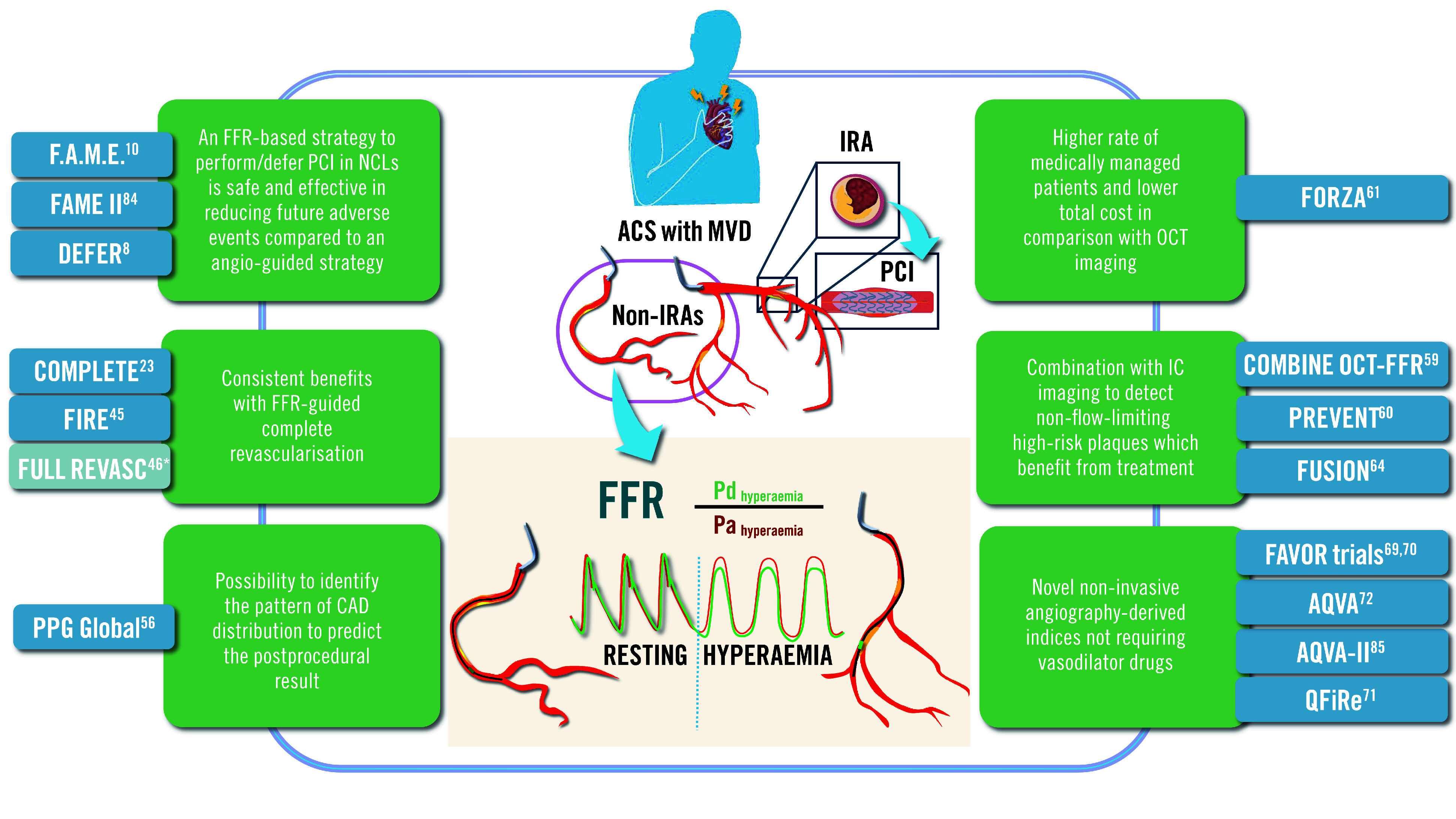
Multivessel coronary artery disease (CAD), defined as ≥50% stenosis in 2 or more epicardial arteries, is associated with a high burden of morbidity and mortality in acute coronary syndrome (ACS) patients. A salient challenge for managing this cohort is selecting the optimal revascularisation strategy, for which the use of coronary physiology has been increasingly recognised. Fractional flow reserve (FFR) is an invasive, pressure wire-based, physiological index measuring the functional significance of coronary lesions. Understanding this can help practitioners evaluate which lesions could induce myocardial ischaemia and, thus, decide which vessels require urgent revascularisation. Non-hyperaemic physiology-based indices, such as instantaneous wave-free ratio (iFR), provide valid alternatives to FFR. While FFR and iFR are recommended by international guidelines in stable CAD, there is ongoing discussion regarding the role of physiology in patients with ACS and multivessel disease (MVD); growing evidence supports FFR use in the latter. Compelling findings show FFR-guided complete percutaneous coronary intervention (PCI) can reduce adverse cardiovascular events, mortality, and repeat revascularisations in ACS and MVD patients compared to angiography-based PCI. However, FFR is limited in identifying non-flow-limiting vulnerable plaques, which can disadvantage high-risk patients. Here, integrating coronary physiology assessment with intracoronary imaging in decision-making can improve outcomes and quality of life. Further research into novel physiology-based tools in ACS and MVD is needed. This review aims to highlight the key evidence surrounding the role of FFR and other functional indices in guiding PCI strategy in ACS and MVD patients.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
-
- Park DW, Clare RM, Schulte PJ, Pieper KS, Shaw LK, Califf RM, Ohman EM, Van de, Hirji S, Harrington RA, Armstrong PW, Granger CB, Jeong MH, Patel MR. Extent, location, and clinical significance of non-infarct-related coronary artery disease among patients with ST-elevation myocardial infarction. JAMA. 2014;312:2019–27. - PubMed
-
- Sorajja P, Gersh BJ, Cox DA, McLaughlin MG, Zimetbaum P, Costantini C, Stuckey T, Tcheng JE, Mehran R, Lansky AJ, Grines CL, Stone GW. Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur Heart J. 2007;28:1709–16. - PubMed
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407–77. - PubMed
-
- Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, Bittl JA, Cohen MG, DiMaio JM, Don CW, Fremes SE, Gaudino MF, Goldberger ZD, Grant MC, Jaswal JB, Kurlansky PA, Mehran R, Metkus TS, Nnacheta LC, Rao SV, Sellke FW, Sharma G, Yong CM, Zwischenberger BA. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e4–17. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous