

Neurological sequelae after childhood bacterial meningitis
- PMID: 39347811
- PMCID: PMC11527958
- DOI: 10.1007/s00431-024-05788-w
Neurological sequelae after childhood bacterial meningitis
Abstract
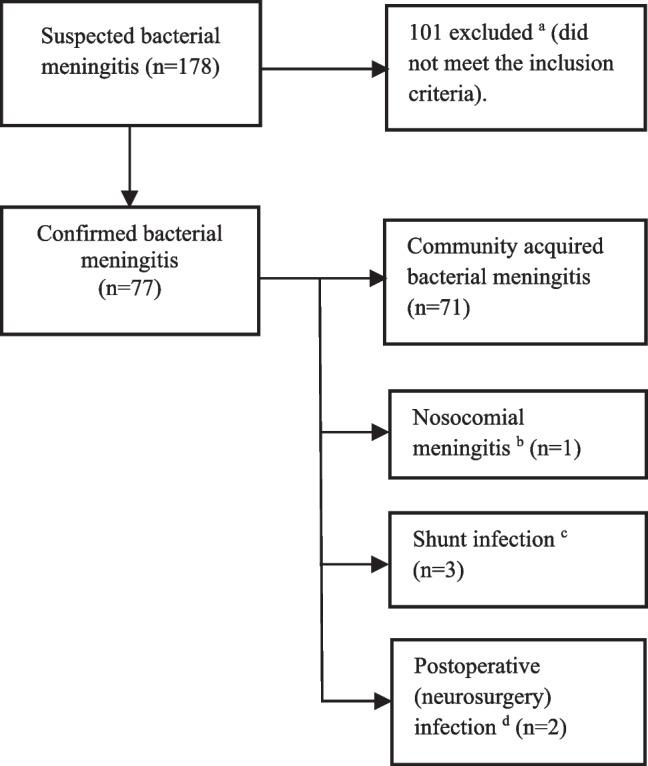
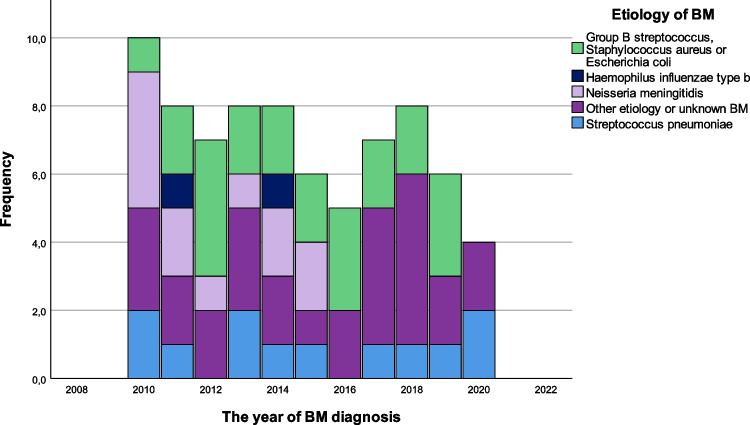
The purpose of this study is to evaluate childhood bacterial meningitis (BM): incidence, clinical presentation, causative pathogens, diagnostics, and outcome (neurological sequelae, hearing loss, and death). A retrospective review of all children aged ≤ 16 years and 1 month diagnosed with BM at a tertiary children's centre in the period 2010-2020. The Glasgow Outcome Scale (GOS) was used to assess outcome, with a GOS score of 1-4 considered to be an unfavourable outcome. Logistic regression univariate analysis was used to determine predefined risk factors for death, unfavourable outcome, and long-term neurological sequelae. Seventy-four patients (44 males) with a median age of 8.0 months (range 1 day to 16 years and 1 month) and 77 BM episodes were included in the study. The average incidence rate of BM was 2.2/100,000/year, the majority (91%) being community-acquired BM. Streptococcus pneumonia and Neisseria meningitidis were the most common pathogens 12/77 (16%) each. Neurological sequelae at discharge were present in 24 (34%) patients, unfavourable outcome in 19 (25%), and hearing loss (deafness) in two (3%) survivors of BM. Seven (9%) patients died. Long-term neurological sequelae were observed in 19/60 (32%), aphasia/dysphasia being the most common in 10 (17%) BM children. No independent risk factors were identified for long-term neurological sequelae in univariate analysis.
Conclusion: The risk for a fatal course of BM is still remarkable. Neurological sequelae persisted in a substantial proportion of BM survivors in long-term follow-up, aphasia/dysphasia being the most common. Hearing loss (deafness) occurred in 3%. However, no specific risk factors predicting the long-term sequelae were found.
What is known: • Streptococcus pneumonia and Neisseria meningitidis were the most common pathogens causing bacterial meningitis. • Risk for fatal course of bacterial meningitis (BM) remains remarkable despite advances in modern medicine.
What is new: • In long-term follow-up, 1/3 of BM children suffered from neurological sequelae in the 2010s, aphasia and dysphasia being the most common sequelae. • Hearing loss was diagnosed in only two (3%) children, whom of both were deaf.
Keywords: Bacterial meningitis; Child; Deafness; Death; Hearing loss; Neurological sequelae.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Neurological sequelae remain frequent after bacterial meningitis in children.Acta Paediatr. 2020 Feb;109(2):361-367. doi: 10.1111/apa.14942. Epub 2019 Aug 11. Acta Paediatr. 2020. PMID: 31325195
-
Hearing impairment after childhood bacterial meningitis dependent on etiology in Luanda, Angola.Int J Pediatr Otorhinolaryngol. 2015 Nov;79(11):1820-6. doi: 10.1016/j.ijporl.2015.08.015. Epub 2015 Aug 22. Int J Pediatr Otorhinolaryngol. 2015. PMID: 26357930
-
Sequelae after bacterial meningitis in childhood.Scand J Infect Dis. 2002;34(5):379-82. doi: 10.1080/00365540110080179. Scand J Infect Dis. 2002. PMID: 12069024
-
Early neurologic complications and long-term sequelae of childhood bacterial meningitis in a limited-resource country (Kosovo).Childs Nerv Syst. 2013 Feb;29(2):275-80. doi: 10.1007/s00381-012-1917-3. Epub 2012 Sep 12. Childs Nerv Syst. 2013. PMID: 22968209 Review.
-
Long-term sequelae of childhood bacterial meningitis: an underappreciated problem.Pediatr Infect Dis J. 2011 Jan;30(1):3-6. doi: 10.1097/INF.0b013e3181ef25f7. Pediatr Infect Dis J. 2011. PMID: 20683377 Review.
References
-
- Nigrovic LE, Kuppermann N, Malley R (2008) Children with bacterial meningitis presenting to the emergency department during the pneumococcal conjugate vaccine era. Acad Emerg Med 15(6):522–528. 10.1111/j.1553-2712.2008.00117.x - PubMed
-
- Thigpen MC, Whitney CG, Messonnier NE et al (2011) Bacterial meningitis in the United States, 1998–2007. N Engl J Med 364(21):2016–2025. 10.1056/NEJMoa1005384 - PubMed
-
- Chavez-Bueno S, McCracken Jr GH. Bacterial meningitis in children. Pediatr Clin North Am. 2005;52(3):795–810, vii. S0031–3955(05)00038–6 [pii] - PubMed
-
- Svendsen MB, Ring Kofoed I, Nielsen H, Schønheyder HC, Bodilsen J (2020) Neurological sequelae remain frequent after bacterial meningitis in children. Acta Paediatr 109(2):361–367. 10.1111/apa.14942 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
