

Computer modeling and validation testing for glenoid component rotation and optimal glenoid screw angles for reverse shoulder arthroplasty in an Asian population
- PMID: 39347986
- PMCID: PMC11564314
- DOI: 10.1007/s00264-024-06340-z
Computer modeling and validation testing for glenoid component rotation and optimal glenoid screw angles for reverse shoulder arthroplasty in an Asian population
Abstract
Purpose: Good initial fixation of glenoid component for reverse total shoulder arthroplasty (RTSA) relies on component placement and screw purchase in the scapula bone. This is especially difficult in an Asian population with small glenoid geometry. Optimal glenoid component roll angle and screw angulation to achieve the longest screws for best fixation has not been defined in the current literature.
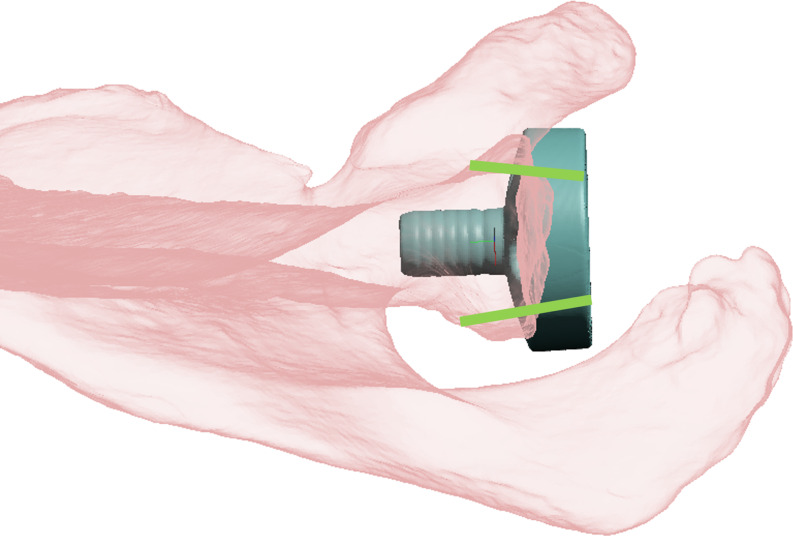
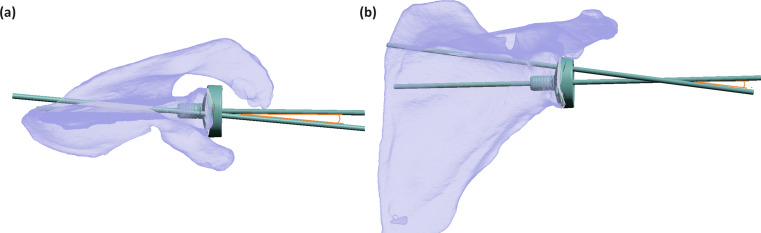
Methods: Computer 3D modelling of 133 scapulas with RTSA performed were analyzed to determine patient specific optimal glenoid roll angle (GRA) for the longest bi-cortical screws attainable. The cranial-caudal angle (CCA), anterior-posterior angle (APA) and lengths for the superior and inferior screws were measured. Validation testing using calculated average (CA) angles and rounded average (RA) angles to the nearest 5 degree were recomputed for each case to determine the bi-cortical screw lengths achievable. The CA and RA screw lengths were compared against patient specific modelling using paired-sample t-tests.
Results: Average GRA was - 1.6°, almost perpendicular to the long axis of the glenoid and achieves an average bi-cortical screw length of 51.3 mm and 45.5 mm for the superior and inferior screws respectively. The CCA and APA were 9.1° cranial and 6.5° posterior for the superior screw and screw angulation of 11.2° caudal and 0.7° anterior for the inferior screw. Validation testing shows statistically shorter screw lengths in the CA and RA models compared to patient specific modelling (p < 0.01).
Conclusion: Validation testing with average angles for GRA, CCA and APA demonstrates strong patient heterogeneity and anatomical variation. Despite this, screw lengths attainable in the RA group were > 38 mm with good safety profile. Surgeons may consider the additional use of navigation-assisted, or 3D printed patient specific instrumentation to optimize baseplate and screw configuration for RTSA.
Keywords: 3D modelling; Glenoid fixation; Patient specific instrumentation; Reverse shoulder arthroplasty; Screw length.
© 2024. The Author(s).
Conflict of interest statement
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
