

Peripartum cardiomyopathy: a comprehensive and contemporary review
- PMID: 39348083
- PMCID: PMC11455798
- DOI: 10.1007/s10741-024-10435-5
Peripartum cardiomyopathy: a comprehensive and contemporary review
Abstract
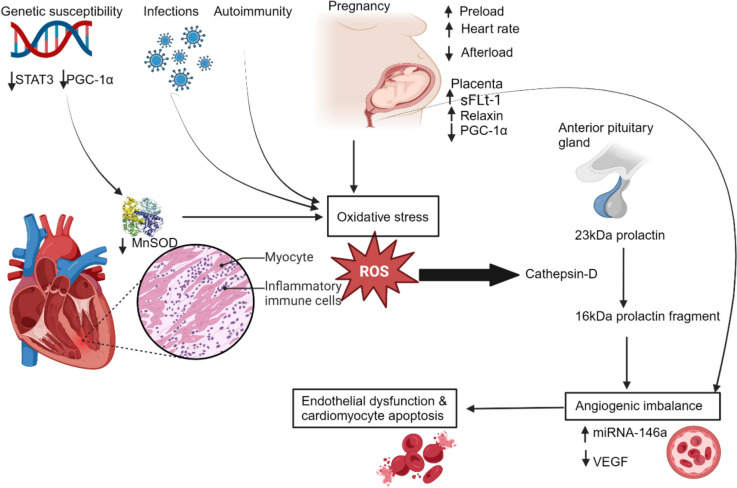
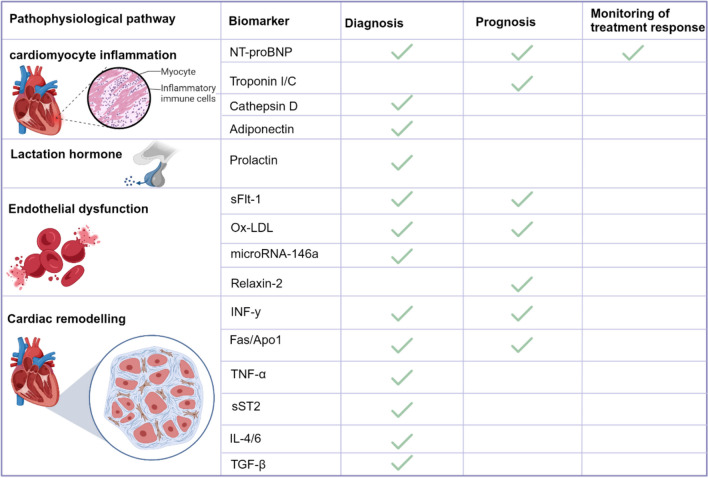
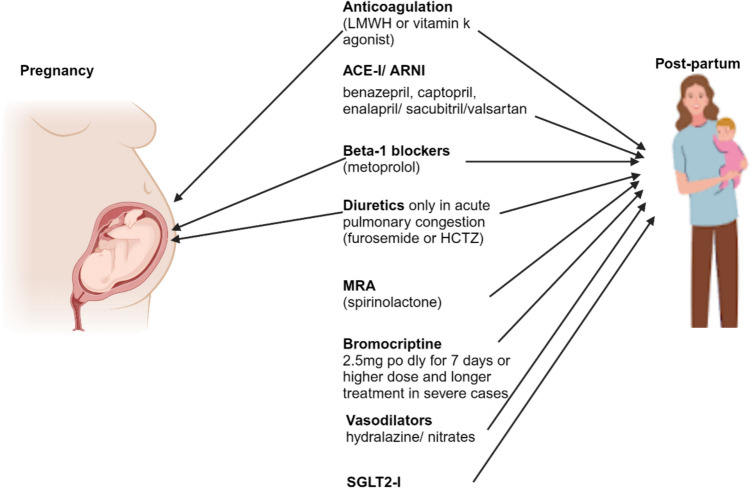
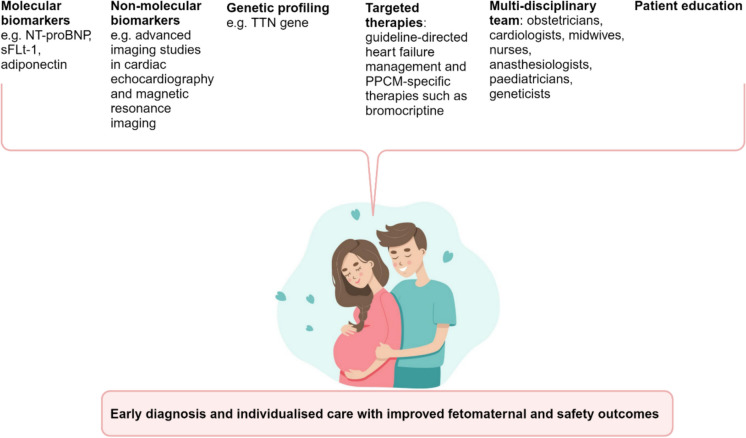
Cardiovascular disease is a major non-communicable disease globally, with increasing prevalence, posing a significant public health challenge. It is the leading non-obstetric cause of perinatal morbidity and mortality, with a substantial number of cardiac fatalities occurring in individuals without any known pre-existing cardiovascular disease. Peripartum cardiomyopathy is a type of de novo heart failure that occurs in pregnant women in the late stages of pregnancy or following delivery. Despite extensive research, diagnosing and managing peripartum cardiomyopathy remains challenging, resulting in significant morbidity and mortality. Recent advancements and novel approaches have been made to better understand and manage peripartum cardiomyopathy, including molecular and non-molecular biomarkers, genetic predisposition and risk prediction, targeted therapies, multidisciplinary care, and improved patient education. This narrative review provides a comprehensive overview and new perspectives on peripartum cardiomyopathy, covering its epidemiology, updated pathophysiological mechanisms, diagnosis, management, and future research directions for healthcare professionals, researchers, and clinicians.
Keywords: Biomarkers; Management; Novel approaches; Pathophysiology; Peripartum cardiomyopathy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ogah OS, Adebiyi AA, Sliwa K (2019) Heart failure in sub-Saharan Africa. https://pdfs.semanticscholar.org
-
- Draper ES, Gallimore ID, Smith LK, et al (2019) Mothers and babies: reducing risk through audits and confidential enquiries across the UK (MBRRACE-UK). Available from https://www.npeu.ox.ac.uk/downloads/files/mbrrace-uk/reports/MBRRACE-UK
-
- Bauersachs J, König T, Van der Meer P, Petrie MC et al (2019) Pathophysiology, diagnosis and management of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. Eur J Heart Fail 21:827–843 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
