

Modulation of diabetes-related retinal pathophysiology by PTX3
- PMID: 39348530
- PMCID: PMC11474045
- DOI: 10.1073/pnas.2320034121
Modulation of diabetes-related retinal pathophysiology by PTX3
Abstract
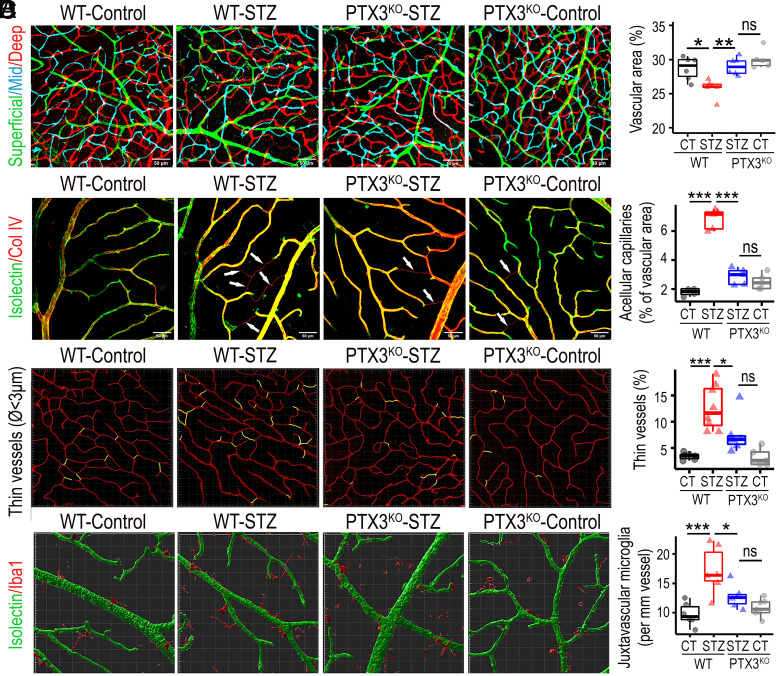
Diabetic retinopathy (DR) is a common complication of diabetes characterized by vascular pathology and neuroinflammation. Pentraxin 3 (PTX3) is a soluble pattern recognition molecule that functions at the crossroads between innate immunity, inflammation, and tissue remodeling. DR is known to involve inflammatory pathways, although the potential relevance of PTX3 has not been explored. We found that PTX3 protein levels increased in the retina of diabetic mice. Similarly, evaluation of a publicly available transcriptomic human dataset revealed increased PTX3 expression in DR with diabetic macular edema and proliferative retinopathy, when compared to nondiabetic retinas or diabetic retinas without complications. To further understand the role of PTX3 within DR, we employed the streptozotocin-induced diabetes model in PTX3 knockout mice (PTX3KO), which were followed up for 9 mo to evaluate hallmarks of disease progression. In diabetic PTX3KO mice, we observed decreased reactive gliosis, diminished microglia activation, and reduced vasodegeneration, when compared to diabetic PTX3 wild-type littermates. The decrease in DR-associated pathological features in PTX3KO retinas translated into preserved visual function, as evidenced by improved optokinetic response, restored b-wave amplitude in electroretinograms, and attenuated neurodegeneration. We showed that PTX3 induced an inflammatory phenotype in human retinal macroglia, characterized by GFAP upregulation and increased secretion of IL6 and PAI-1. We confirmed that PTX3 was required for TNF-α-induced reactive gliosis, as PTX3KO retinal explants did not up-regulate GFAP in response to TNF-α. This study reveals a unique role for PTX3 as an enhancer of sterile inflammation in DR, which drives pathogenesis and ultimately visual impairment.
Keywords: PTX3; diabetic retinopathy; gliosis; microglia; retinopathy.
Conflict of interest statement
Competing interests statement:The authors declare no competing interest.
Figures





References
-
- Guariguata L., et al. , Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 103, 137–149 (2014). - PubMed
-
- Leasher J. L., et al. , Global estimates on the number of people blind or visually impaired by diabetic retinopathy: A meta-analysis from 1990 to 2010. Diabetes Care 39, 1643–1649 (2016). - PubMed
-
- Noma H., Mimura T., Yasuda K., Shimura M., Role of inflammation in diabetic macular edema. Ophthalmologica 232, 127–135 (2014). - PubMed
MeSH terms
Substances
Grants and funding
- Science Forum Proof of Principle Award/Novo Nordisk (Novo Nordisk Global)
- BB/T000805/1/UKRI | Biotechnology and Biological Sciences Research Council (BBSRC)
- MR/S036695/1/UKRI | Medical Research Council (MRC)
- 20/0006162/DUK_/Diabetes UK/United Kingdom
- MacularSociety RPG2022/Macular Society (The Macular Society)
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
