

Spatial single-cell profiling and neighbourhood analysis reveal the determinants of immune architecture connected to checkpoint inhibitor therapy outcome in hepatocellular carcinoma
- PMID: 39349005
- PMCID: PMC11874287
- DOI: 10.1136/gutjnl-2024-332837
Spatial single-cell profiling and neighbourhood analysis reveal the determinants of immune architecture connected to checkpoint inhibitor therapy outcome in hepatocellular carcinoma
Abstract
Background: The determinants of the response to checkpoint immunotherapy in hepatocellular carcinoma (HCC) remain poorly understood. The organisation of the immune response in the tumour microenvironment (TME) is expected to govern immunotherapy outcomes but spatial immunotypes remain poorly defined.
Objective: We hypothesised that the deconvolution of spatial immune network architectures could identify clinically relevant immunotypes in HCC.
Design: We conducted highly multiplexed imaging mass cytometry on HCC tissues from 101 patients. We performed in-depth spatial single-cell analysis in a discovery and validation cohort to deconvolute the determinants of the heterogeneity of HCC immune architecture and develop a spatial immune classification that was tested for the prediction of immune checkpoint inhibitor (ICI) therapy.
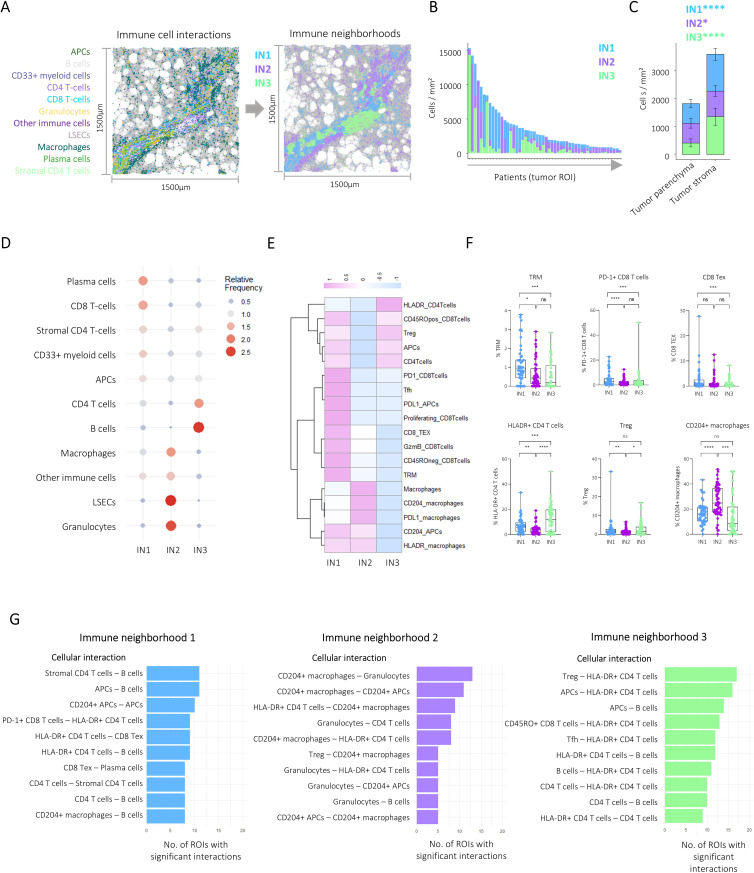
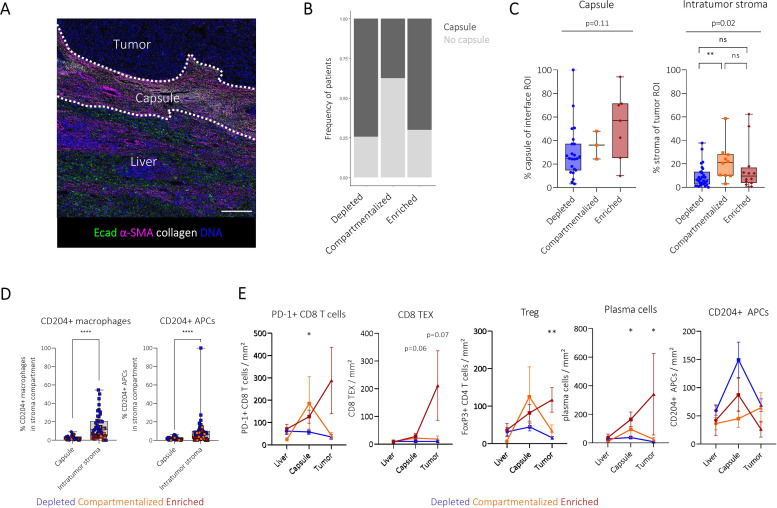
Results: Bioinformatic analysis identified 23 major immune, stroma, parenchymal and tumour cell types in the HCC TME. Unsupervised neighbourhood detection based on the spatial interaction of immune cells identified three immune architectures with differing involvement of immune cells and immune checkpoints dominated by either CD8 T-cells, myeloid immune cells or B- and CD4 T-cells. We used these to define three major spatial HCC immunotypes that reflect a higher level of intratumour immune cell organisation: depleted, compartmentalised and enriched. Progression-free survival under ICI therapy differed significantly between the spatial immune types with improved survival of enriched patients. In patients with intratumour heterogeneity, the presence of one enriched area governed long-term survival.
Keywords: CANCER IMMUNOBIOLOGY; HEPATOCELLULAR CARCINOMA; IMAGE ANALYSIS; IMMUNOTHERAPY; LIVER IMMUNOLOGY.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures





References
-
- Ducreux M, Abou-Alfa GK, Bekaii-Saab T, et al. The management of hepatocellular carcinoma. Current expert opinion and recommendations derived from the 24th ESMO/World Congress on Gastrointestinal Cancer, Barcelona, 2022. ESMO Open. 2023;8:101567. doi: 10.1016/j.esmoop.2023.101567. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials