

Effects of implementation strategies on nursing practice and patient outcomes: a comprehensive systematic review and meta-analysis
- PMID: 39350295
- PMCID: PMC11443951
- DOI: 10.1186/s13012-024-01398-0
Effects of implementation strategies on nursing practice and patient outcomes: a comprehensive systematic review and meta-analysis
Abstract
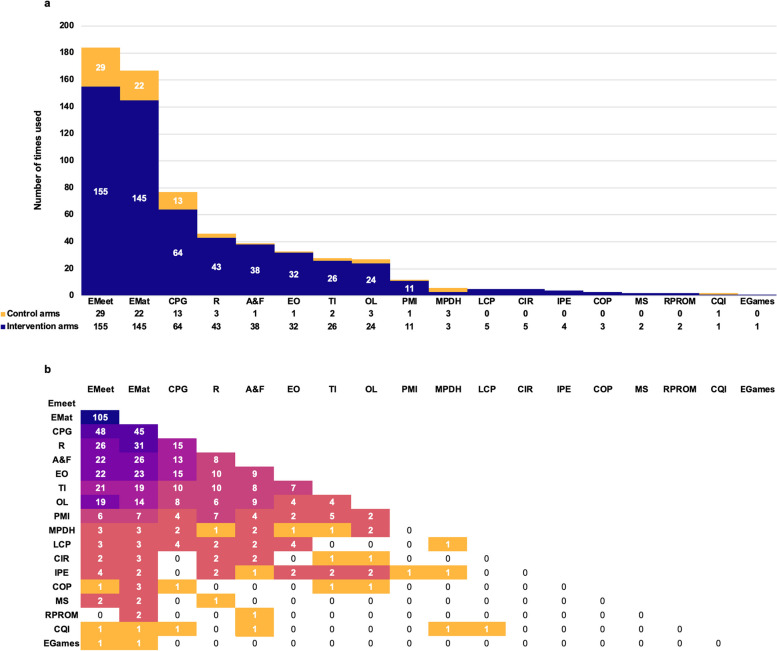
Background: Implementation strategies targeting individual healthcare professionals and teams, such as audit and feedback, educational meetings, opinion leaders, and reminders, have demonstrated potential in promoting evidence-based nursing practice. This systematic review examined the effects of the 19 Cochrane Effective Practice and Organization Care (EPOC) healthcare professional-level implementation strategies on nursing practice and patient outcomes.
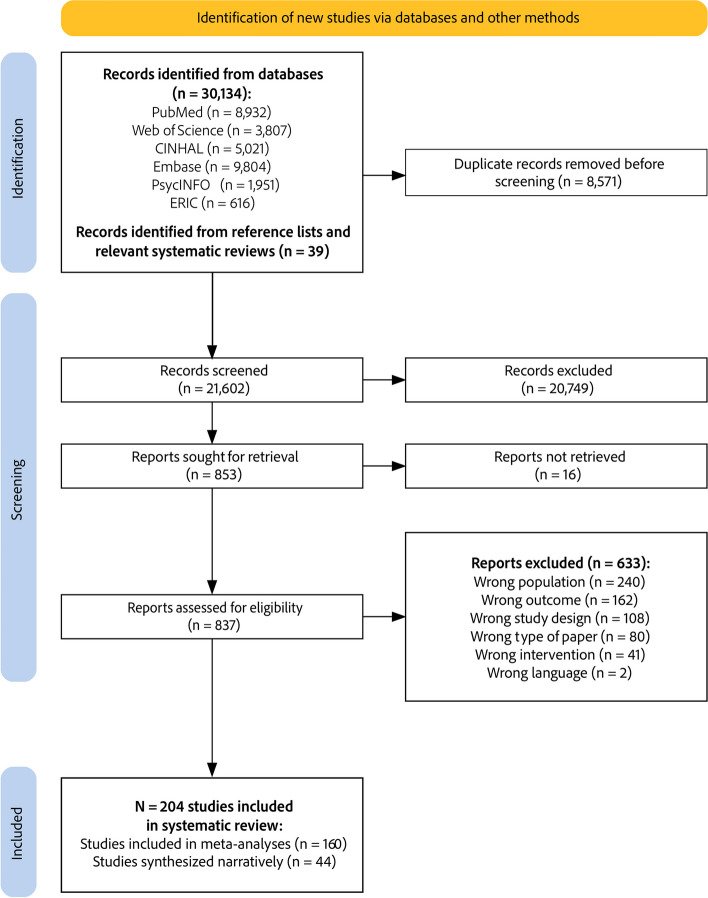
Methods: A systematic review was conducted following the Cochrane Handbook, with six databases searched up to February 2023 for randomized studies and non-randomized controlled studies evaluating the effects of EPOC implementation strategies on nursing practice. Study selection and data extraction were performed in Covidence. Random-effects meta-analyses were conducted in RevMan, while studies not eligible for meta-analysis were synthesized narratively based on the direction of effects. The quality of evidence was assessed using GRADE.
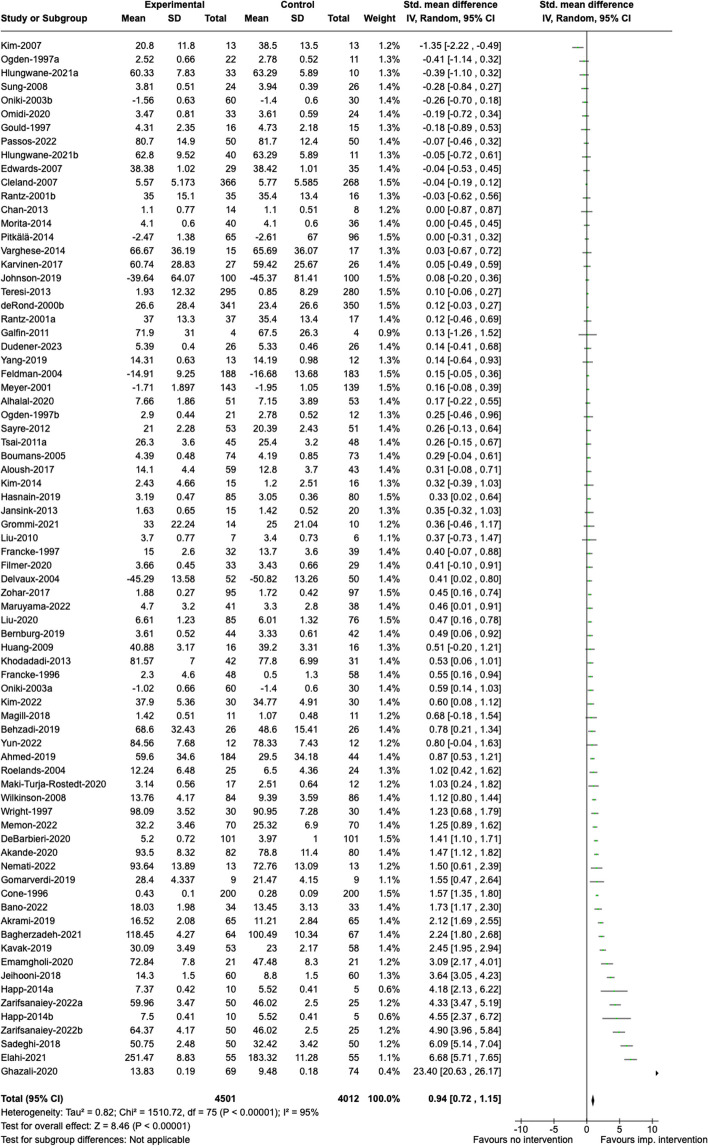
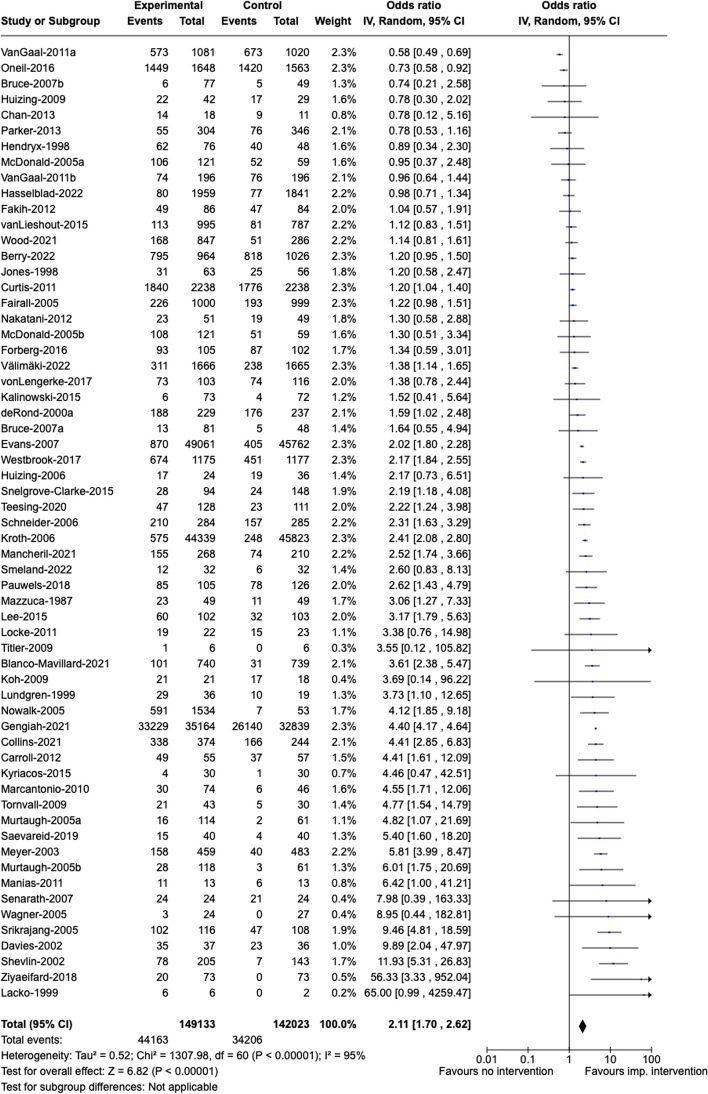
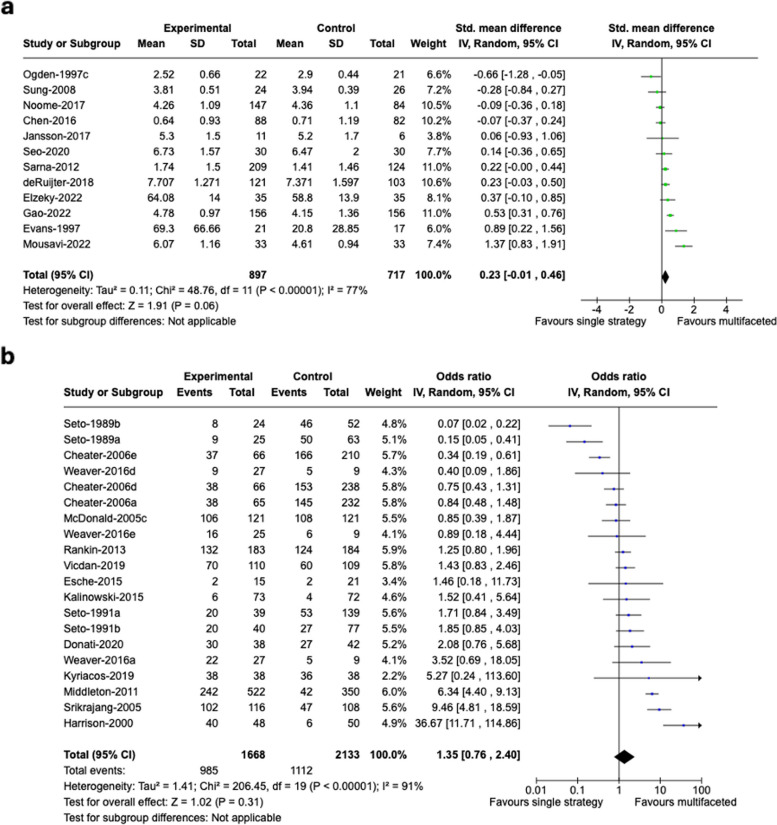
Results: Out of 21,571 unique records, 204 studies (152 randomized, 52 controlled, non-randomized) enrolling 36,544 nurses and 340,320 patients were included. Common strategies (> 10% of studies) were educational meetings, educational materials, guidelines, reminders, audit and feedback, tailored interventions, educational outreach, and opinion leaders. Implementation strategies as a whole improved clinical practice outcomes compared to no active intervention, despite high heterogeneity. Group and individual education, patient-mediated interventions, reminders, tailored interventions and opinion leaders had statistically significant effects on clinical practice outcomes. Individual education improved nurses' attitude, knowledge, perceived control, and skills, while group education also influenced perceived social norms. Although meta-analyses indicate a small, non-statistically significant effect of multifaceted versus single strategies on clinical practice, the narrative synthesis of non-meta-analyzed studies shows favorable outcomes in all studies comparing multifaceted versus single strategies. Group and individual education, as well as tailored interventions, had statistically significant effects on patient outcomes.
Conclusions: Multiple types of implementation strategies may enhance evidence-based nursing practice, though effects vary due to strategy complexity, contextual factors, and variability in outcome measurement. Some evidence suggests that multifaceted strategies are more effective than single component strategies. Effects on patient outcomes are modest. Healthcare organizations and implementation practitioners may consider employing multifaceted, tailored strategies to address local barriers, expand the use of underutilized strategies, and assess the long-term impact of strategies on nursing practice and patient outcomes.
Trial registration: PROSPERO CRD42019130446.
Keywords: Clinical practice; Healthcare professional behavior; Implementation strategies; Knowledge translation strategies; Nurses; Nursing practice; Patient outcomes; Professional practice; Quality improvement.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- World Health Organization. State of the world’s nursing 2020: investing in education, jobs and leadership. 2020.
-
- World Health Organization. Global strategic directions for nursing and midwifery 2021–2025. 2021.
-
- United Nations. Transforming our world: the 2030 Agenda for Sustainable Development - Resolution adopted by the General Assembly on 25 September 2015. 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
