

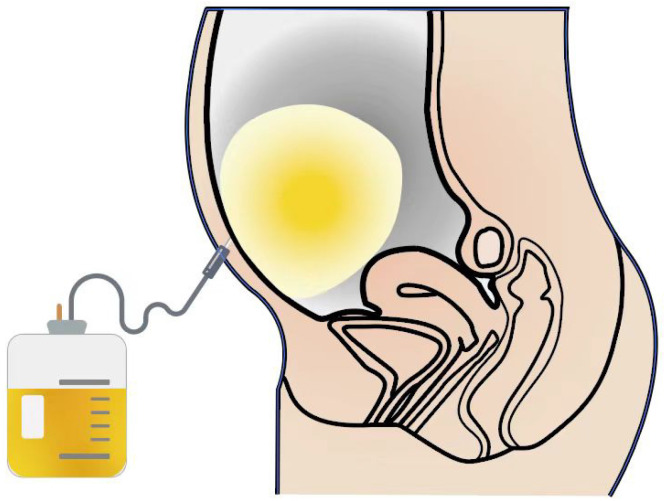
Drainage of ascites in cirrhosis
- PMID: 39351514
- PMCID: PMC11438587
- DOI: 10.4254/wjh.v16.i9.1245
Drainage of ascites in cirrhosis
Abstract
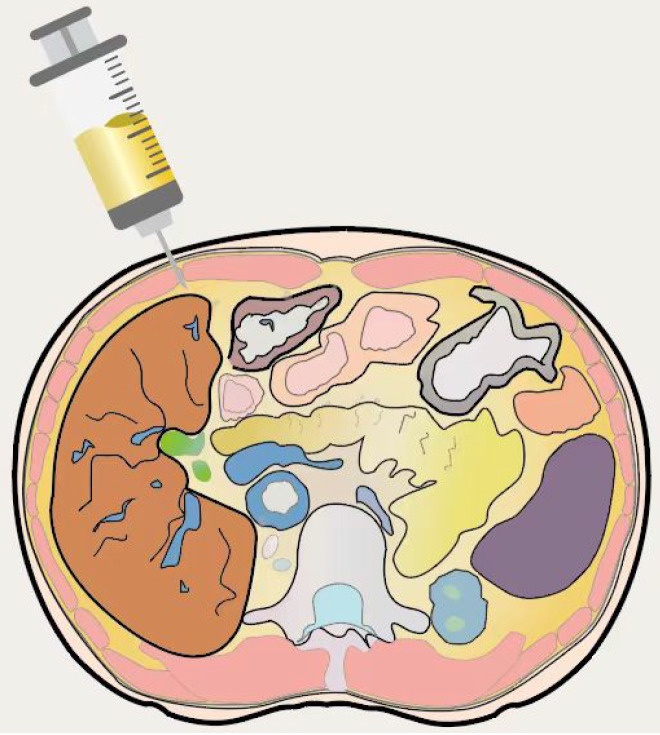
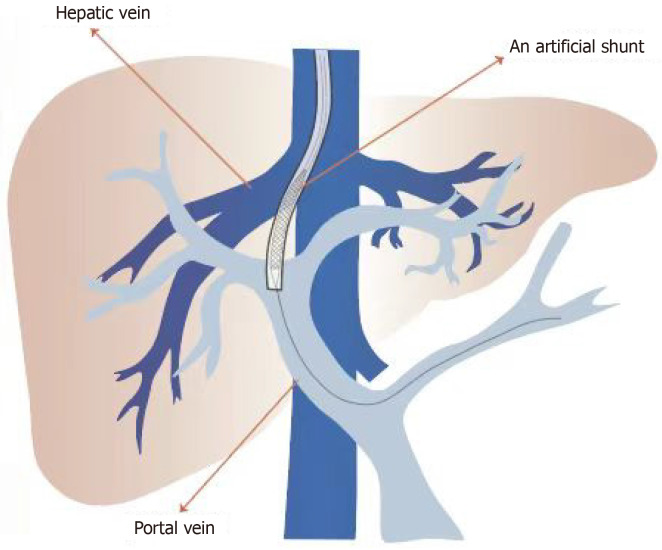
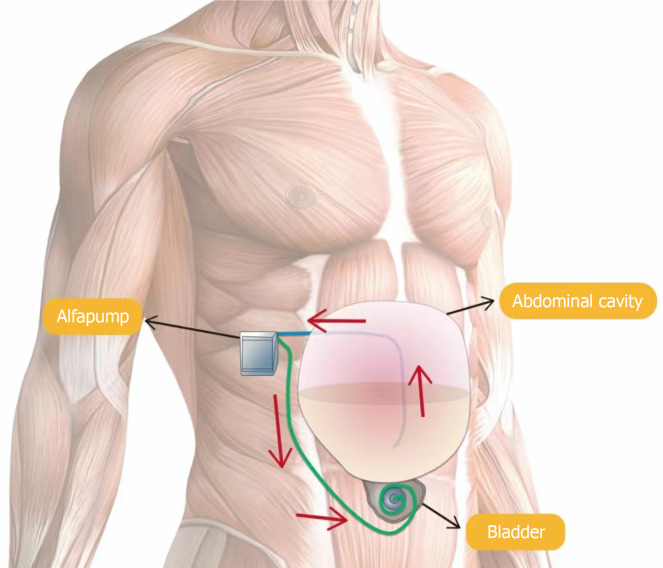
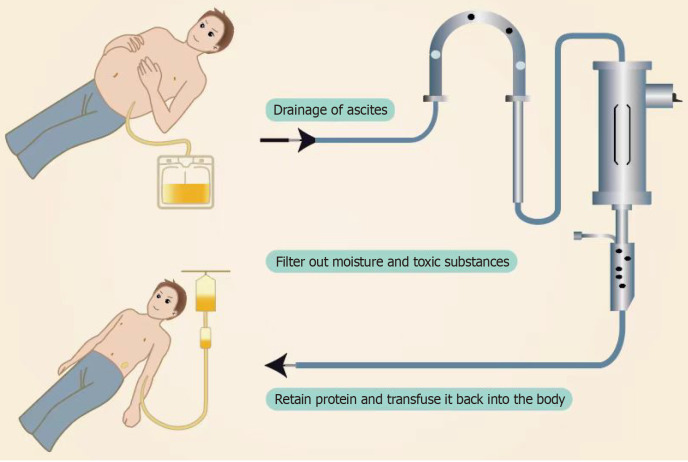
For cirrhotic refractory ascites, diuretics combined with albumin and vasoactive drugs are the first-line choice for ascites management. However, their therapeutic effects are limited, and most refractory ascites do not respond to medication treatment, necessitating consideration of drainage or surgical interventions. Consequently, numerous drainage methods for cirrhotic ascites have emerged, including large-volume paracentesis, transjugular intrahepatic portosystemic shunt, peritoneovenous shunt, automated low-flow ascites pump, cell-free and concentrated ascites reinfusion therapy, and peritoneal catheter drainage. This review introduces the advantages and disadvantages of these methods in different aspects, as well as indications and contraindications for this disease.
Keywords: Automated low-flow ascites pump; Cell-free and concentrated ascites reinfusion therapy; Large-volume paracentesis; Liver cirrhosis ascites; Peritoneal catheter drainage; Peritoneovenous shunt; Transjugular intrahepatic portosystemic shunt.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
References
-
- Bernardi M, Moreau R, Angeli P, Schnabl B, Arroyo V. Mechanisms of decompensation and organ failure in cirrhosis: From peripheral arterial vasodilation to systemic inflammation hypothesis. J Hepatol. 2015;63:1272–1284. - PubMed
-
- Larrue H, Vinel JP, Bureau C. Management of Severe and Refractory Ascites. Clin Liver Dis. 2021;25:431–440. - PubMed
-
- Neong SF, Adebayo D, Wong F. An update on the pathogenesis and clinical management of cirrhosis with refractory ascites. Expert Rev Gastroenterol Hepatol. 2019;13:293–305. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
